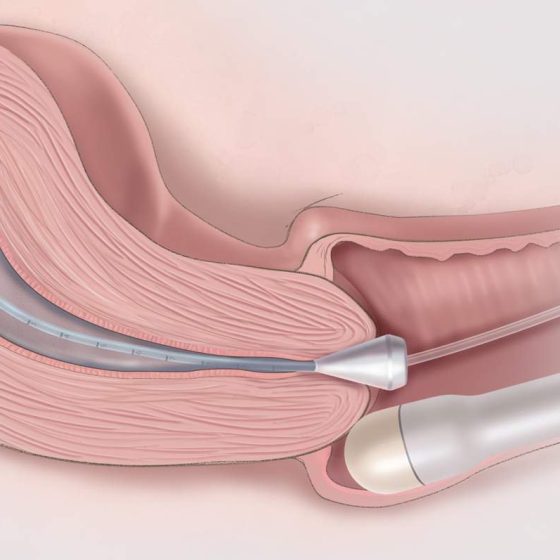
Ultrasound scan of the ovaries
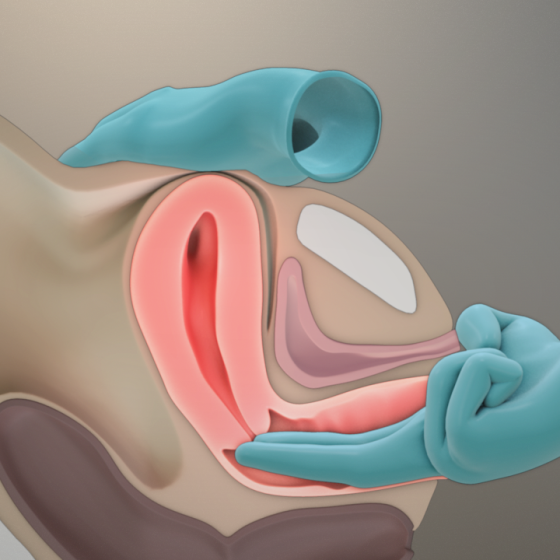
Ultrasound scans use high frequency sound waves to create a picture of a part of the body. It can show the ovaries, womb and surrounding structures. You might have this test to help diagnose ovarian cancer. To have an ultrasound scan of the ovaries, your doctor or radiographer moves a probe over the lower part of your tummy. You may also have an internal vaginal ultrasound. This is when your doctor gently puts the probe into your vagina. This is also called a transvaginal ultrasound scan. We have separate information about what happens during a transvaginal ultrasound scan. Why you have it