Treatment
Medication Therapy
Initial management of cardiogenic shock involves medications to augment the heart’s function. Certain medications, such as dobutamine or milrinone, enhance the heart’s pumping function and are often used first-line to improve the low blood pressure and delivery of blood to the rest of the body.
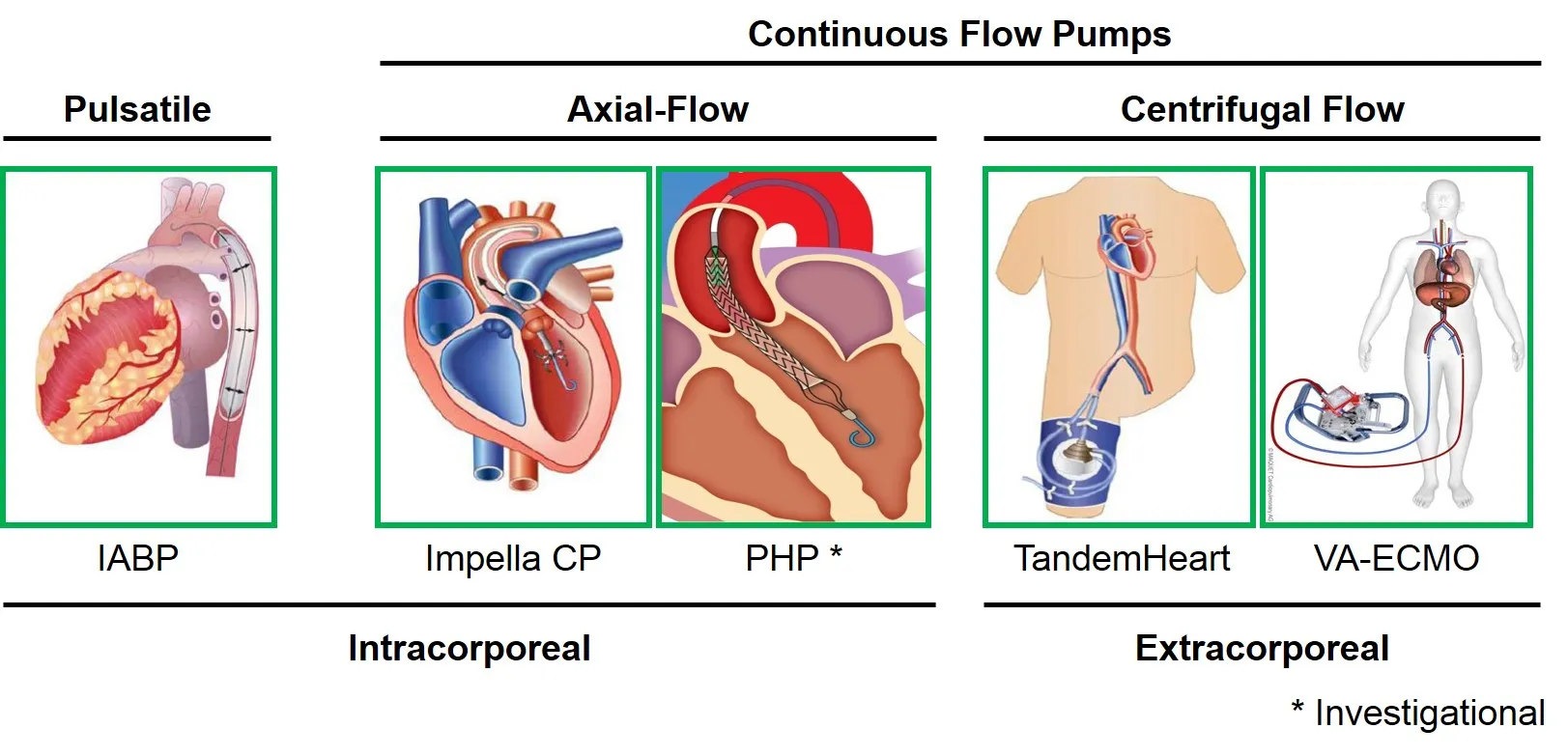
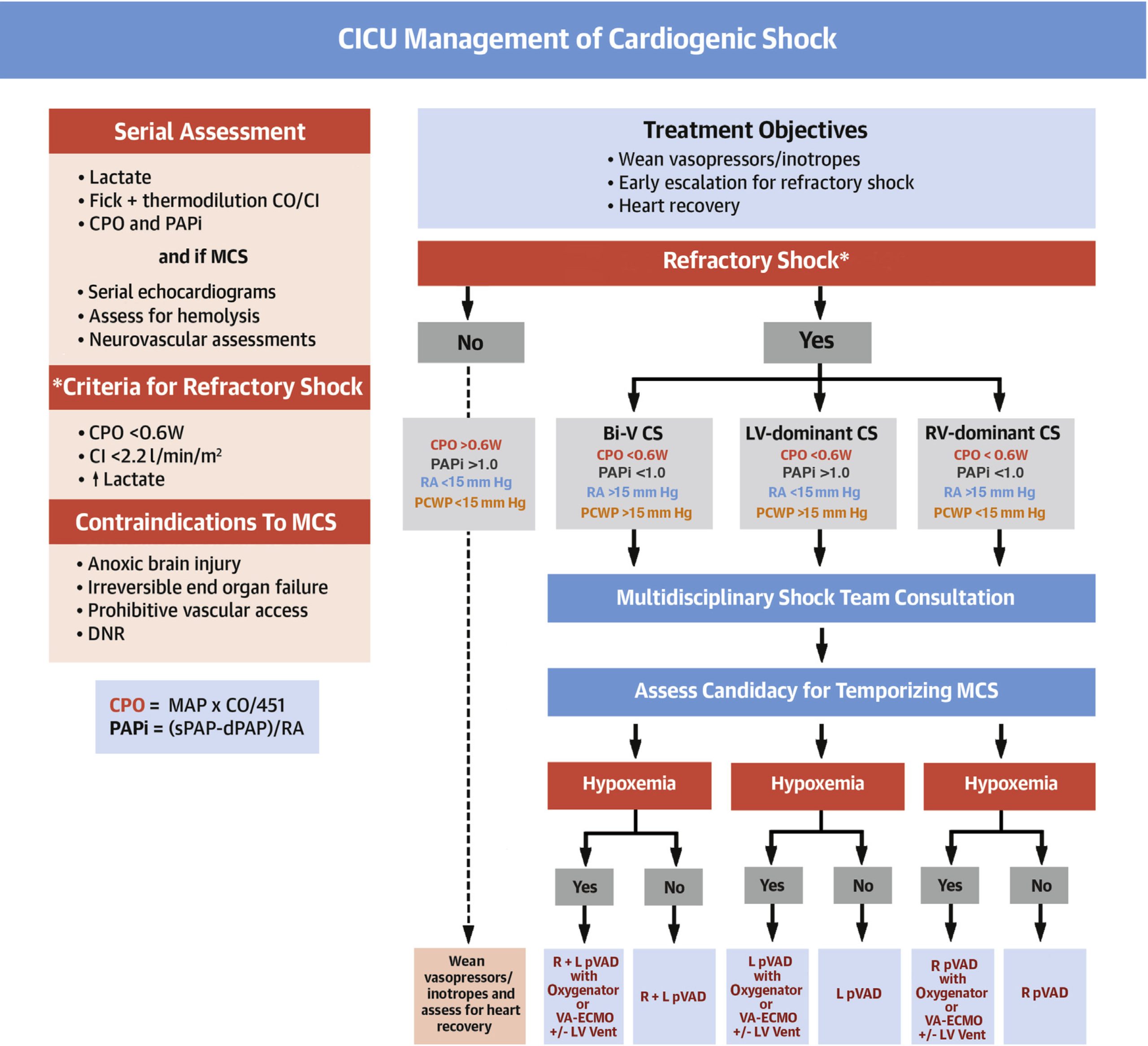
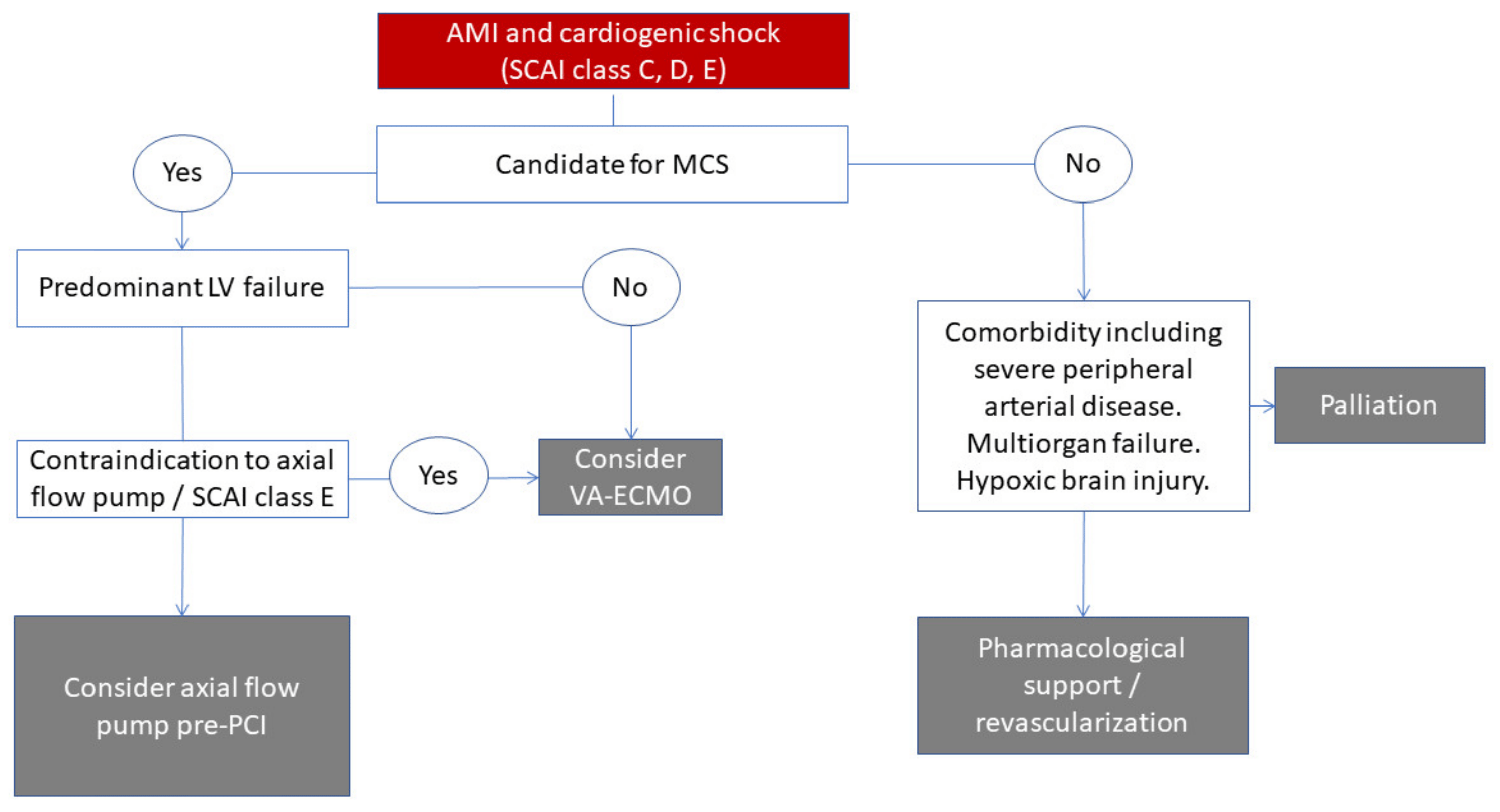
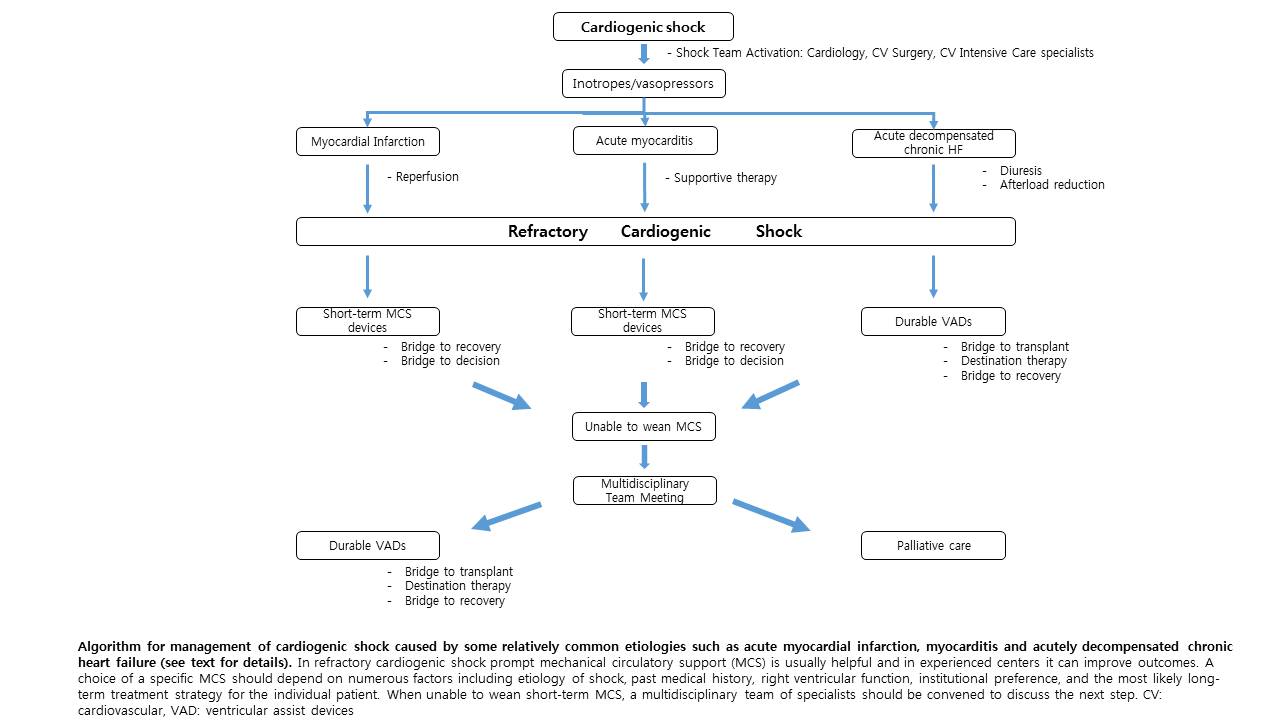
Patients who have cardiogenic shock unresponsive to medication therapy may be candidates for more advanced options such as a mechanical circulatory support device. There are several types of mechanical circulatory support devices, the most common being intra-aortic balloon pumps, left ventricular assist devices, and venous-arterial extra-corporeal membrane oxygenation. It is important to note, however, that none of these devices are permanent solutions but rather are a bridge to a more definitive therapy such as a heart transplantion.
Intra-aortic balloon pump
Main article: Intra-aortic balloon pump
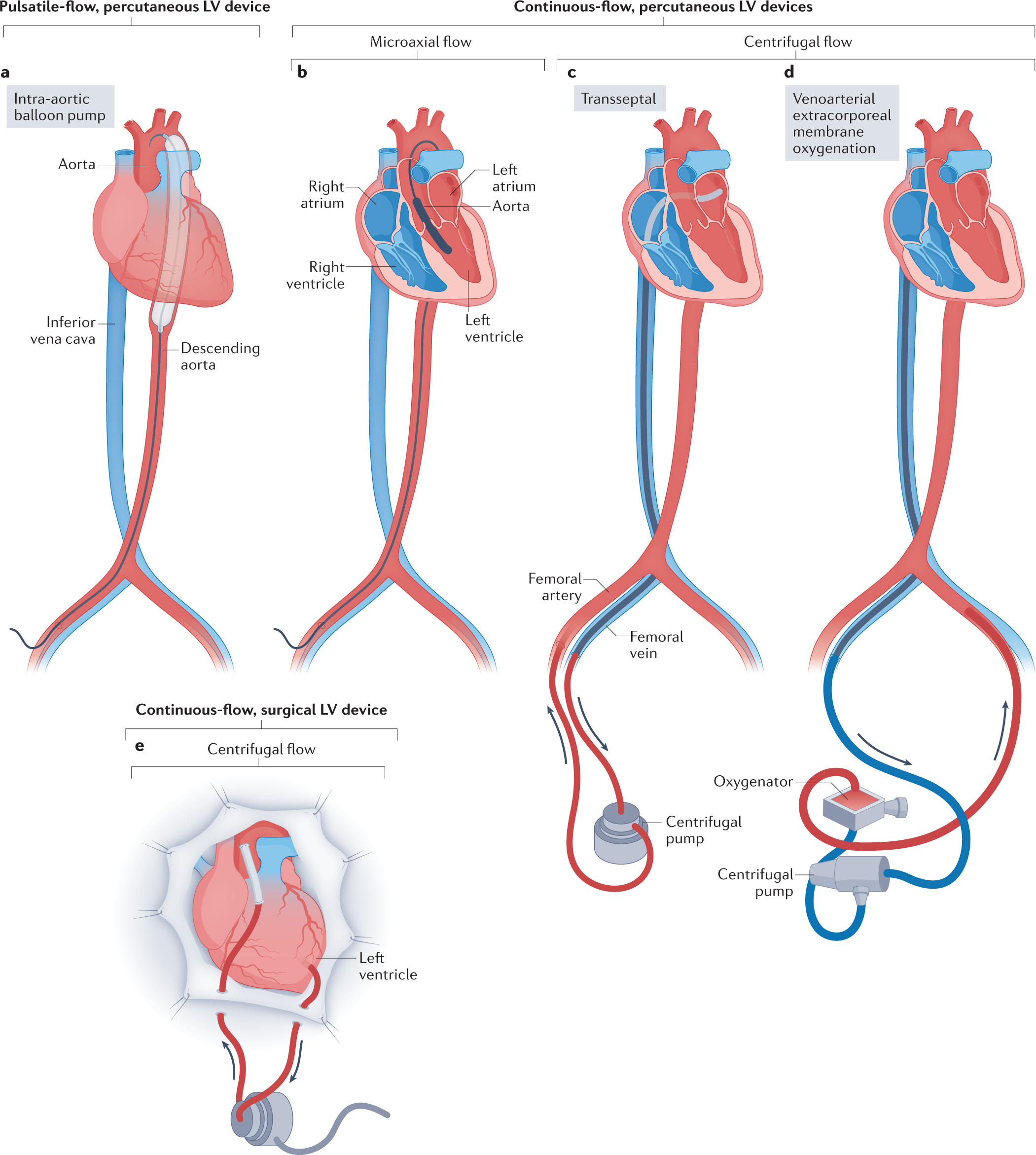
An intra-aortic balloon pump is a device placed by a cardiac surgeon into the descending aorta. It consists of a small balloon filled with helium that helps the heart to pump blood by inflating during diastole (the resting phase of the cardiac cycle) and deflating during systole (the contracting phase of the cardiac cycle). Intra-aortic balloon pumps do not directly increase cardiac output, but importantly, they decrease the amount of pressure that the heart has to pump against, thereby allowing for more blood flow and oxygen to be delivered to the heart muscles.
Intra-aortic balloon pumps have been around for several decades and are most commonly used first-line of the mechanical circulatory support devices. However, it is not without its potential complications. Potential complications include injury upon insertion of the device to arteries supplying the spinal cord as well as risks with any procedure such as bleeding and infection. Contraindications to intra-aortic balloon pumps include aortic dissection, an abdominal aortic aneurysm, and irregularly fast heart beats.
Left ventricular assist device
Main article: Ventricular assist device
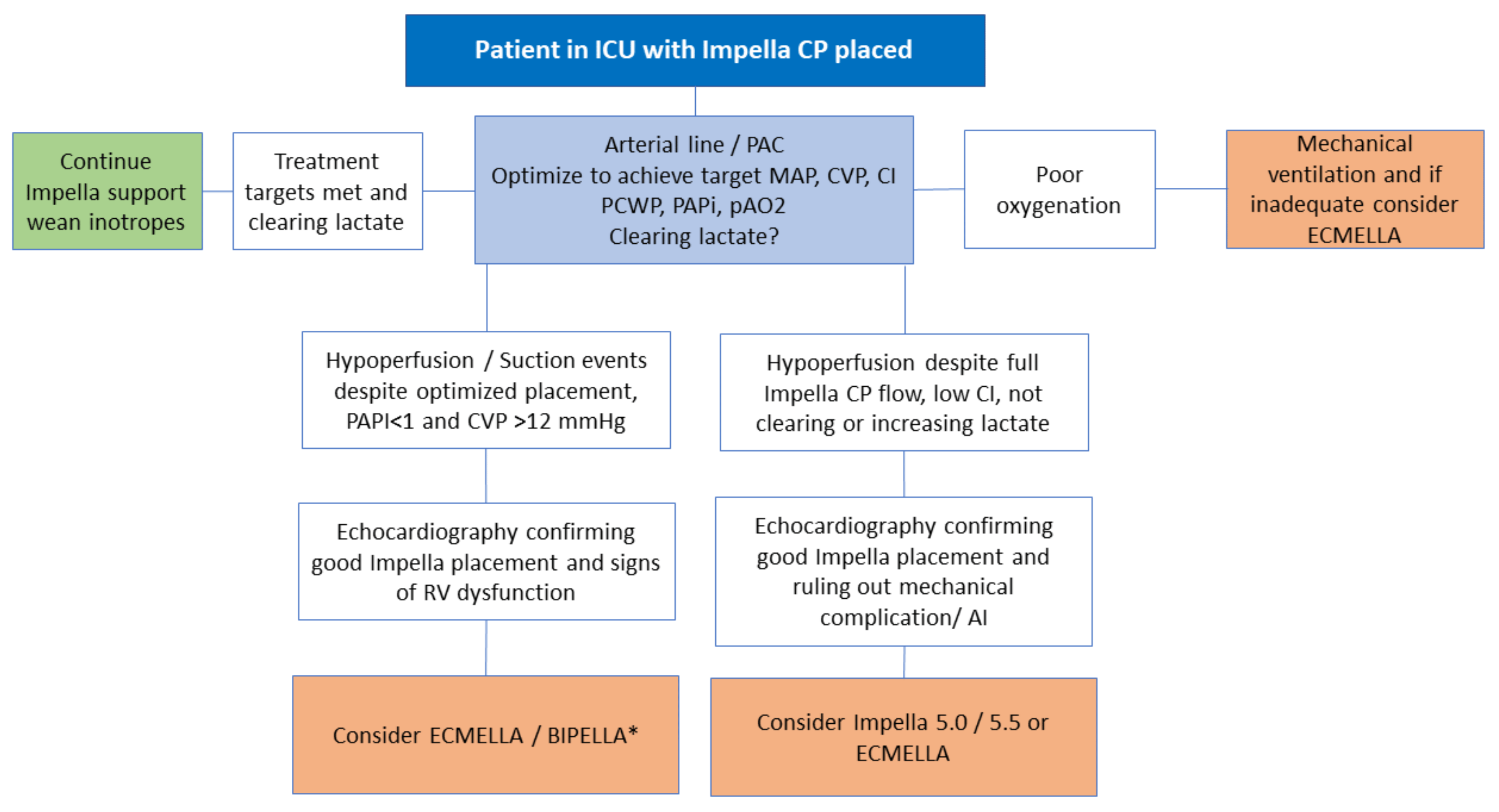
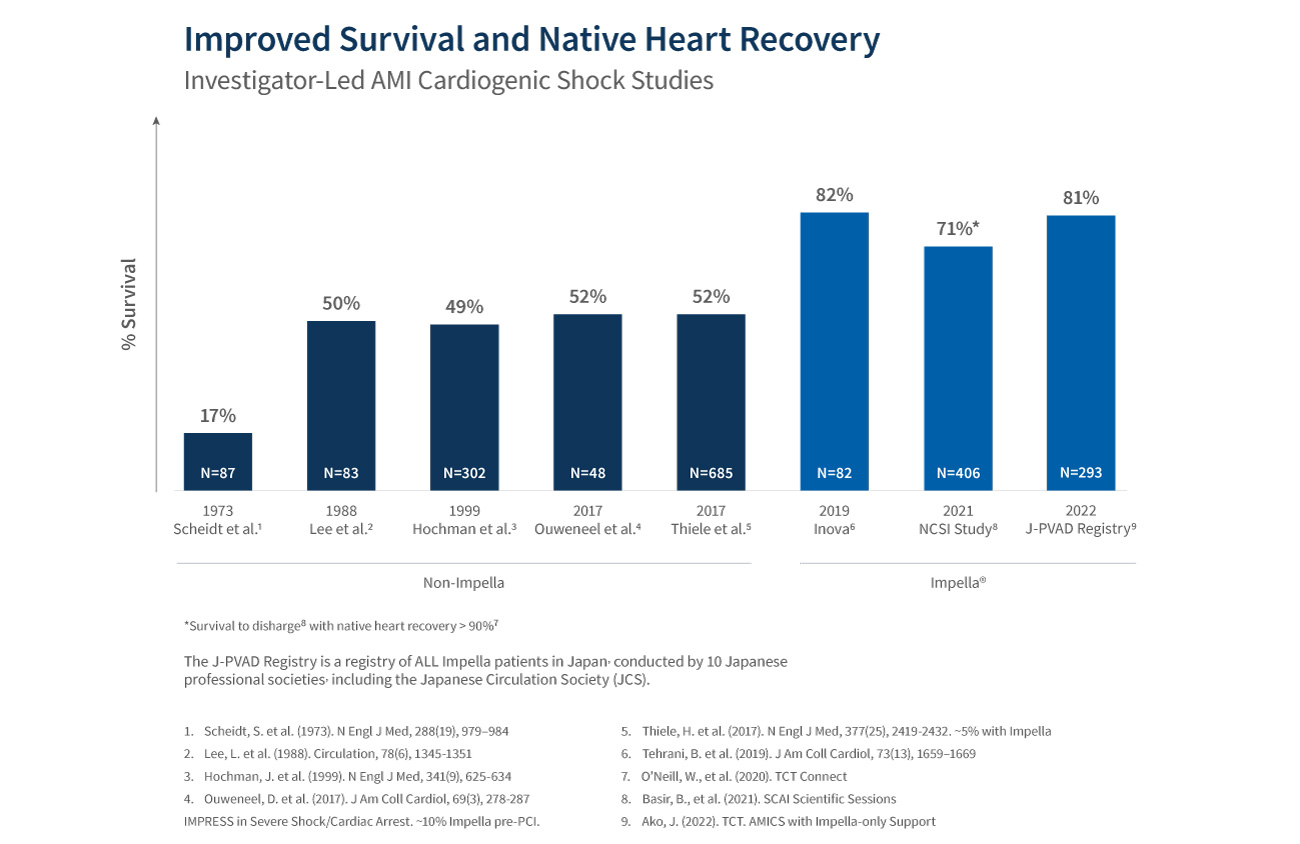
There are several types of left ventricular assist devices, with the Impella devices being some of the most common. This device is placed by a cardiac surgeon into the left ventricle of the heart and essentially acts as a pump, drawing blood from the left ventricle and pushing it out into the aorta so that it could be delivered to the rest of the body. Unlike intra-aortic balloon pumps, the Impella acts independently from the cardiac cycle. It can be adjusted to pump at faster rates to take blood out of the left ventricle and into the aorta more quickly, thereby decreasing the amount of work that the left ventricle has to do. While the Impella is commonly used in settings of cardiogenic shock, some evidence suggests that it placing an Impella device in an acute cardiogenic shock setting, where the heart fails to pump suddenly, may not necessarily guarantee increased survival.
Potential complications specific to an Impella device include hemolysis (shearing of the blood cells) as well as the formation of lesions on the heart valve, namely the mitral or aortic valves. Contraindications to an Impella device insertion include aortic dissection, the presence of a mechanical aortic valve, and the presence of a blood clot in the left ventricle.
Venous-arterial extra-corporeal membrane oxygenation is a circuit support system that is meant to replace the function of the heart as it heals or awaits a more definitive treatment. It consists of a circuit that essentially drains blood from a patient’s venous system, runs that blood through a circulator which adds oxygen and removes carbon dioxide, and ultimately returns blood back into the patient’s arterial system where the newly oxygenated blood can be delivered to the person’s organs. Some evidence suggests that the combination of both an Impella device and Venous-arterial extra-corporeal membrane oxygenation may decrease the heart’s pulmonary capillary wedge pressure, thereby decreasing the amount of stress on the cardiac muscles.
Because Venous-arterial extra-corporeal membrane oxygenation is a very invasive procedure, it is not usually the first-line chosen device for patients in cardiogenic shock and is often reserved only for patients who have not only cardiogenic shock but also respiratory failure and/or concomitant cardiac arrest.
Complications of venous-arterial extra-corporeal membrane oxygenation include an air embolism, pulmonary edema, and blood clotting in the circuit machine.