
Doctors plan your child’s treatment in one of the UK’s children’s cancer centres. Your child has most of their treatment in this specialist centre, but some care might take place at a hospital closer to home.
Children’s cancer centres have teams of specialists who know about Wilms tumours and the best way to treat them. Wilms tumour is curable in about 9 out of 10 children (about 90%).
The main treatments include:
- chemotherapy for almost all children
- surgery for all children
- radiotherapy for some children
In the UK and many other countries, children usually start treatment without having a biopsy  if the tumour looks like a Wilms tumour on the CT or MRI scan. The first treatment is usually chemotherapy. After a few weeks (usually 4 weeks) your child has surgery to remove the tumour. The tumour is looked at under the microscope. Your child’s doctor then makes decisions about further treatment.
if the tumour looks like a Wilms tumour on the CT or MRI scan. The first treatment is usually chemotherapy. After a few weeks (usually 4 weeks) your child has surgery to remove the tumour. The tumour is looked at under the microscope. Your child’s doctor then makes decisions about further treatment.
Decisions about treatment
The specialist team plan treatment according to the type and stage of Wilms tumour your child has. A pathologist looks at the Wilms tumour cells under a microscope. This helps the team decide on the risk group for the tumour. This means if there is a low, medium, or high risk of the cancer coming back after treatment.
They will also look at:
- if your child has a tumour in one or both of their kidneys
- whether there is any spread in the abdomen (tummy area) beyond the kidney (for example to the lymph nodes )
- whether the cancer has spread to distant organs such as the lungs
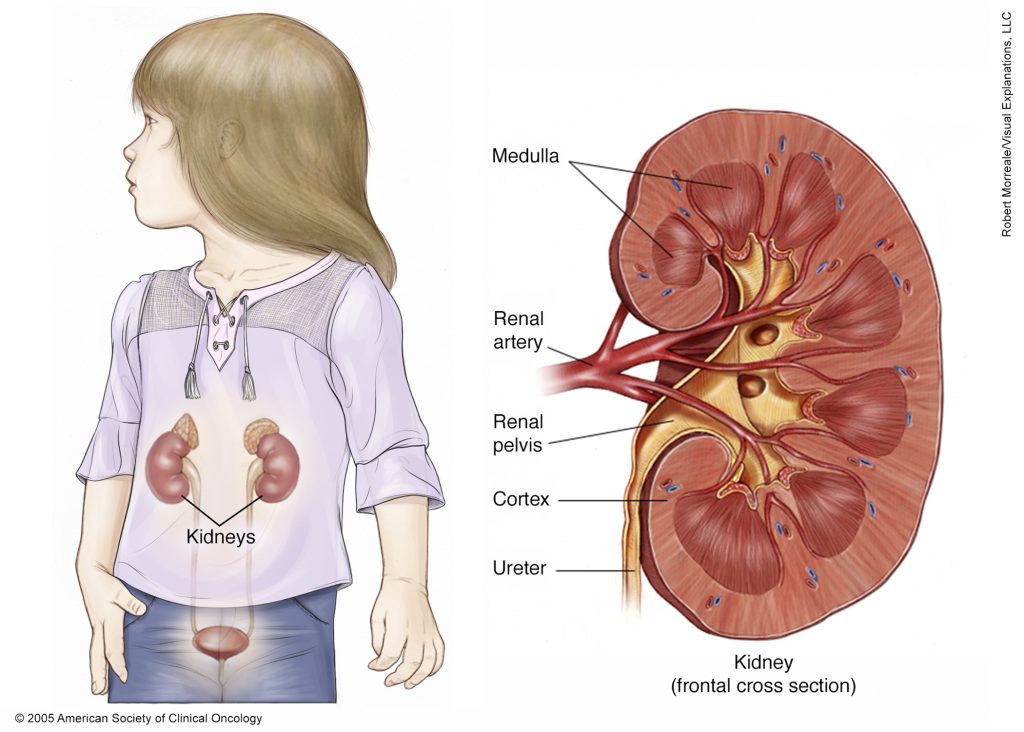
Surgery
After chemotherapy, all children have surgery to remove the affected kidney. This operation is called a nephrectomy.
The surgeon removes the kidney and ususlly some of the tissues around it. The type of surgery for each child is different. The amount of surgery depends on where exactly the tumor is and if other surrounding tissues are involved.
Your child’s surgeon will explain more about your child’s surgery to you.
Most children are in hospital for less than a week. A nephrectomy is a big operation and it can be painful. Your child’s healthcare team will give them regular painkillers to help. After surgery, your child usually has a catheter in place for a short time.



