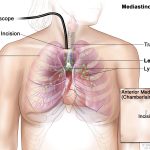
Endoscopic ultrasound combines an ultrasound scan and endoscopy  . It’s also called an endoluminal ultrasound or EUS.
. It’s also called an endoluminal ultrasound or EUS.
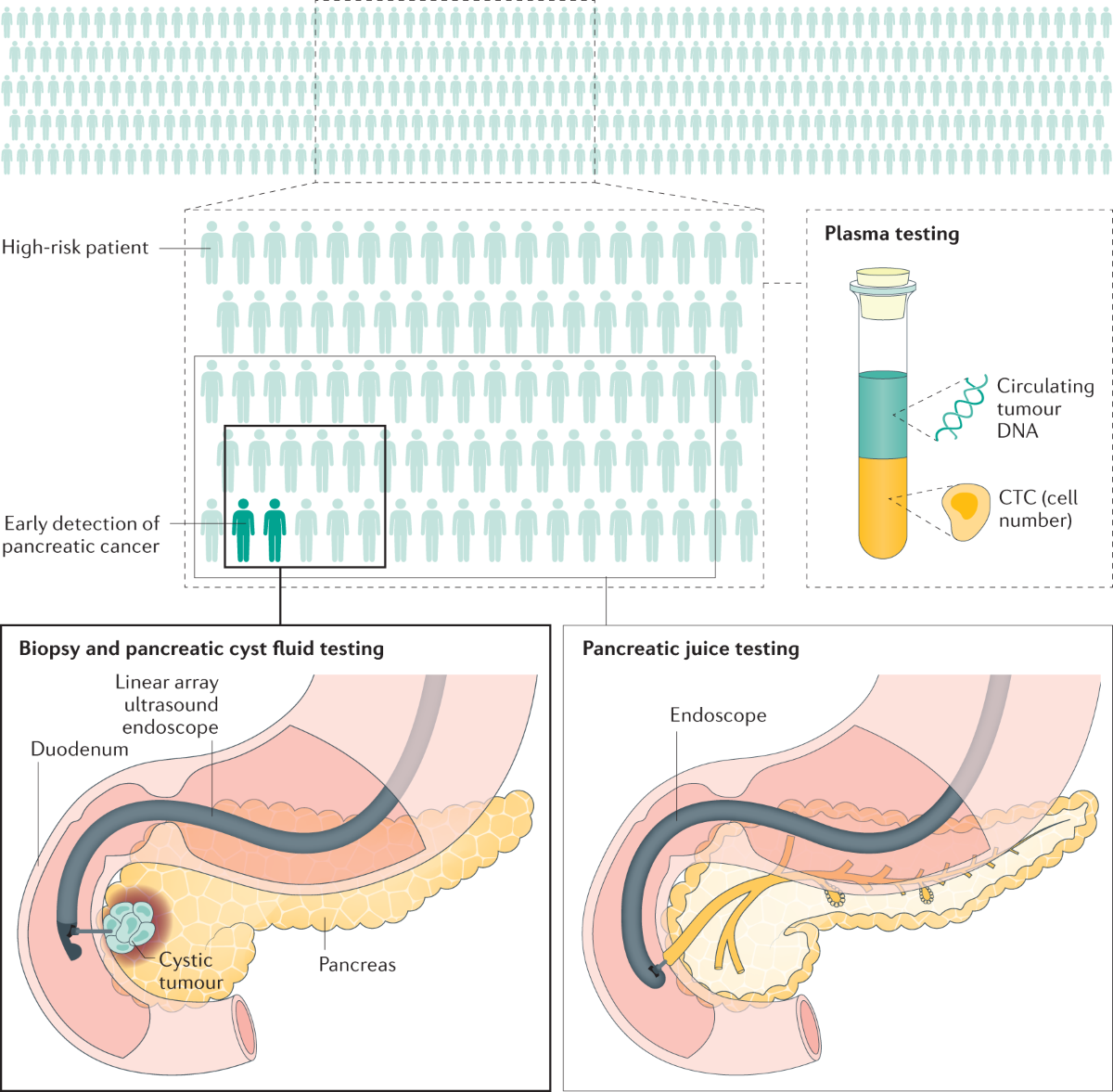
Your doctor or specialist nurse (endoscopist) does the test. They pass a flexible tube called an endoscope into your mouth and down your throat into the stomach. At the end of the endoscope is a small ultrasound probe. The ultrasound picture helps your doctor to see any areas that might be cancer. They can then guide a small needle into these areas to take the biopsy.


This way of taking a biopsy is useful for cancer that has spread to nearby parts of the body such as the liver or peritoneum .
Your doctor can use an ultrasound or CT scan to see exactly where the tumour or tumours are. You have a local anaesthetic injection in the skin over the area so that it goes numb. Your doctor then puts a fine needle through the skin and into the tumour. They can take out a small piece of tissue.
You feel pressure when the needle goes in, but it shouldn’t be painful because of the local anaesthetic.