Mechanics of respiration
The basics of ventilation are simple. To inspire, the intrathoracic pressure must be below that of atmospheric pressure. The reverse must be true in order to expire.
There are two mechanisms by which we may change the intrathoracic volume (and therefore pressure):
- Movement of the diaphragm: the diaphragm is the main muscle of respiration. When it contracts its domes descend expanding the thoracic cavity.
- Movement of the ribcage: The action of various muscles can either move the ribcage up and outward or down and inward.
The muscles of the neck, thorax and abdomen all contribute by causing changes to the volume and, therefore, pressure within the thoracic cavity. Normal breathing, eupnoea, involves the diaphragm and intercostal muscles while forced breathing (during exercise or in disease) requires accessory muscles. This note covers key muscles involved in respiration, it should not be considered an exhaustive list of the muscles involved.
Inspiration
The diaphragm and the external intercostals are the muscles primarily responsible for inspiration. Additional muscles are recruited in active respiration.
Quiet inspiration is a function of two muscles:
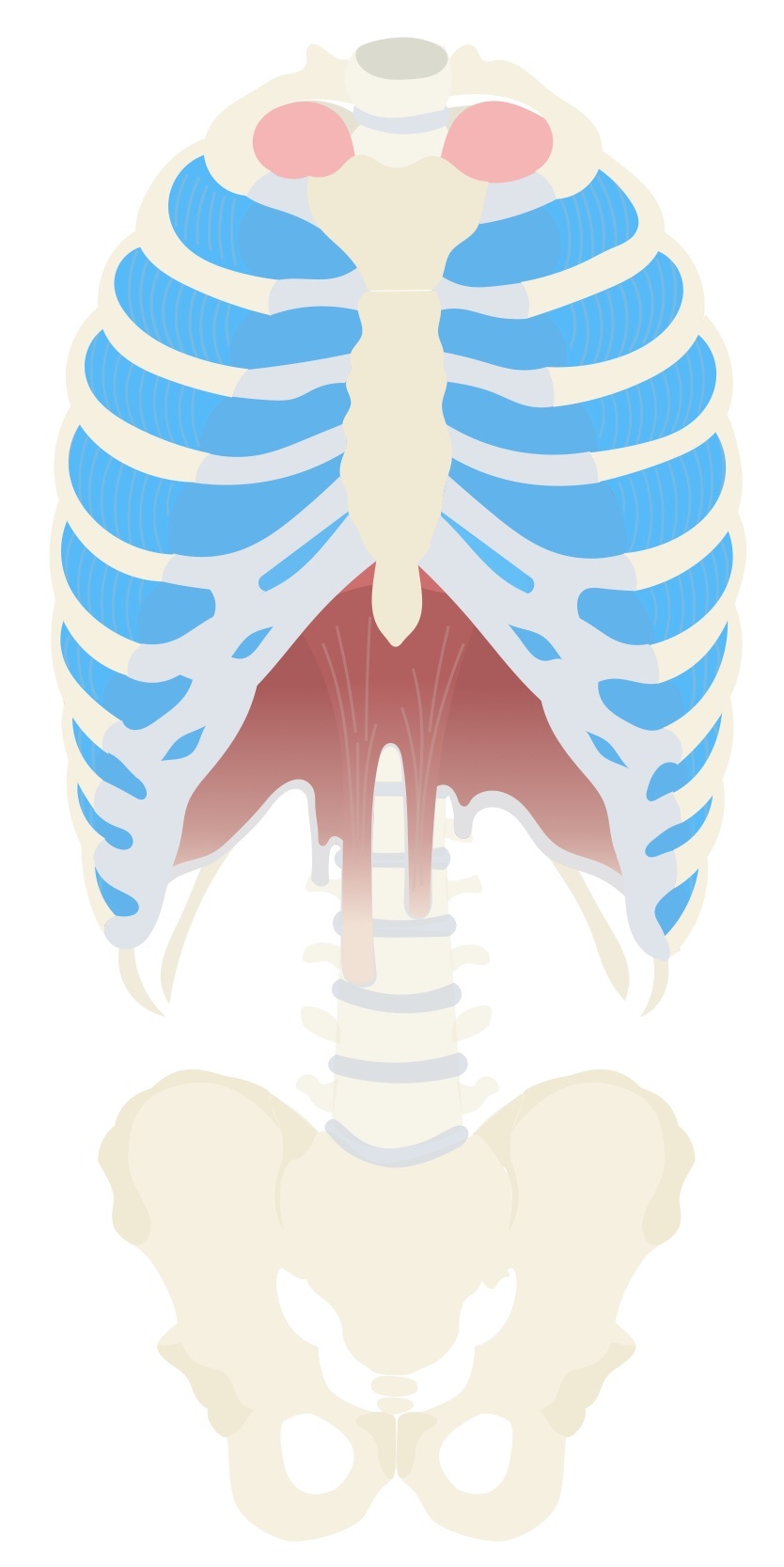
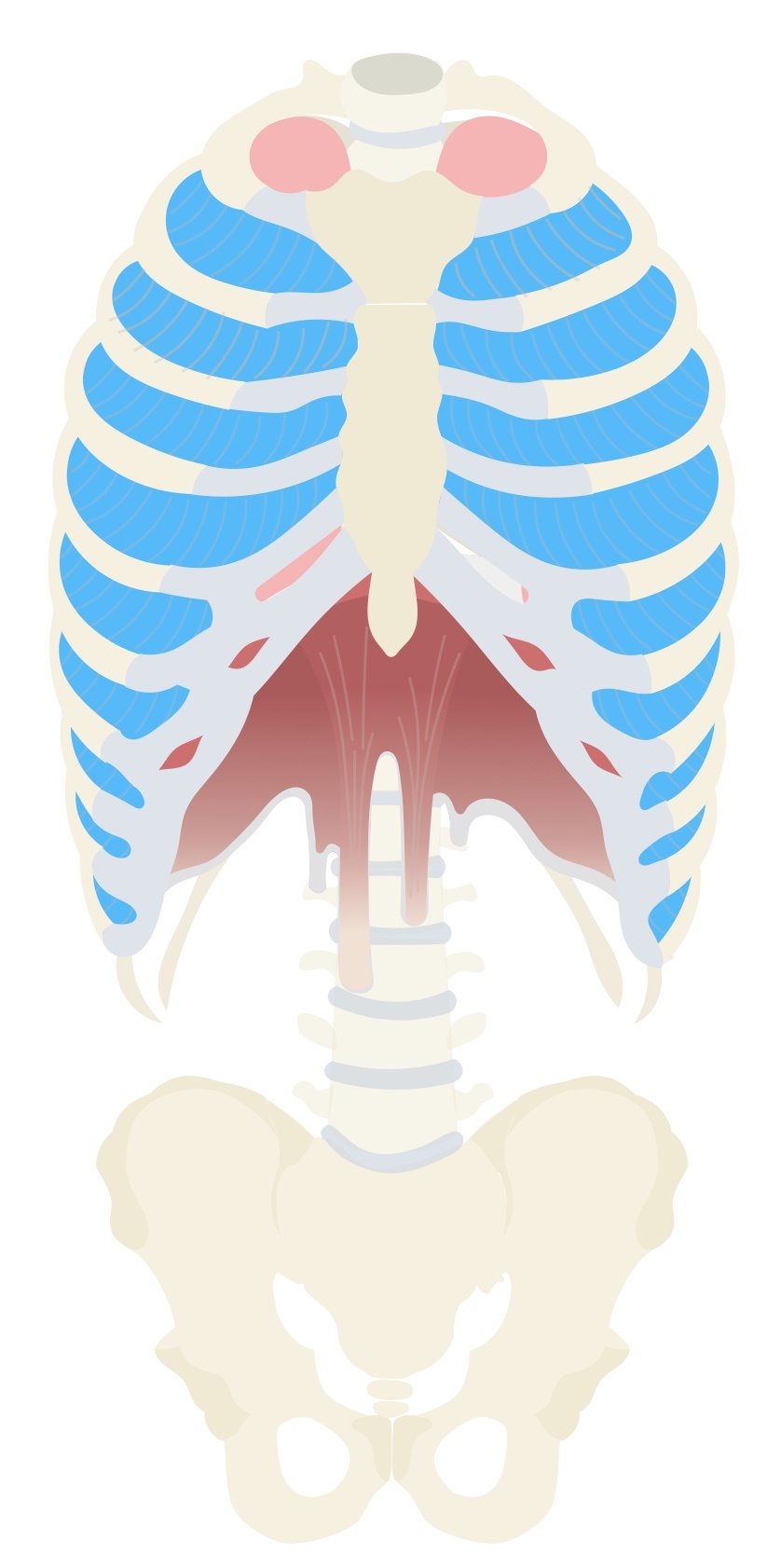
- Diaphragm: A musculotendinous domed structure that divides the thoracic and abdominal cavity. It is the main muscle of respiration. As it contracts it moves down increasing the volume of the thoracic cavity, this results in air being drawn in down its pressure gradient. This contributes 75% of the increase in thoracic volume.
- External intercostals: The external intercostals contribute to quiet inspiration. They cause the ribcage to move up and outward contributing to around 25% of the increase in thoracic volume.
During active or forced inspiration a number of additional ‘accessory’ muscles may be recruited including the sternocleidomastoids and scalenes.
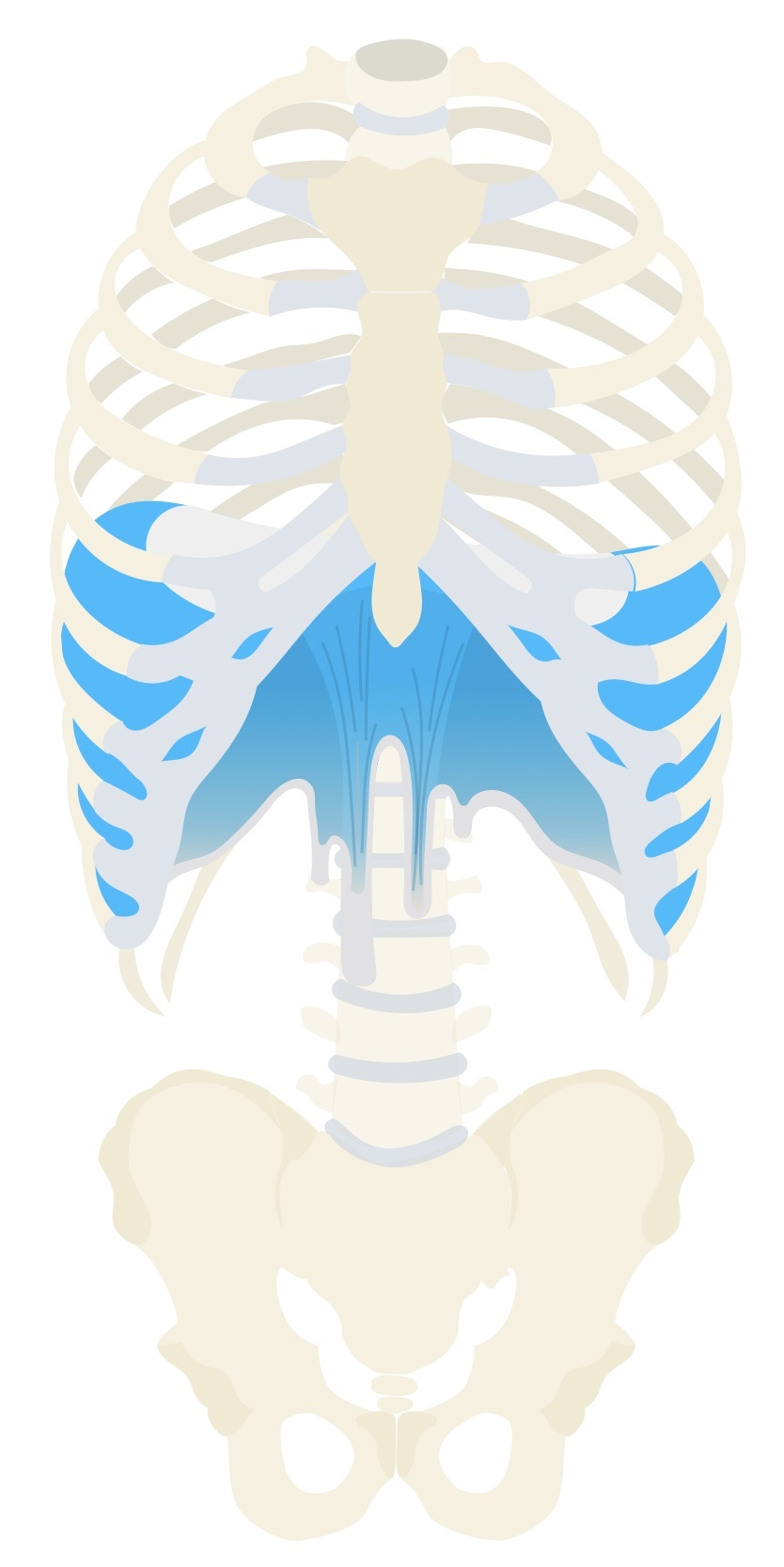
Diaphragm
The diaphragm is a musculotendinous structure that separates the thoracic and abdominal cavities. It is the muscle that is primarily responsible for respiration.
When the diaphragm contracts both domes descend, expanding the thoracic cavity. This increase in volume causes a drop in intrathoracic pressure, drawing air in. At the same time, it increases the intra-abdominal pressure. The combination of raised intra-abdominal pressure and reduced intrathoracic pressure ‘sucks’ venous blood to the heart aiding venous return.
During normal breathing, the diaphragm may only move by 1.5cm, during deep breathing this may increase to 7cm.
Structure
The diaphragm is a double-domed structure with the muscular fibres blending into a central tendon. The surrounding muscular component is divided into three parts:
- Sternal: two muscular slips which attach to the posterior aspect of the xiphoid process.
- Costal: attach to the inferior six ribs and costal cartilages.
- Lumbar: arises from lumbar vertebrae 1-3 and the medial and lateral arcuate ligaments.
The right dome is typically higher due to the presence of the liver below.
Vascular supply and innervation
The diaphragm is innervated by the phrenic nerve, which arises from the spinal nerve roots C3, C4 and C5. This can be remembered using the phrase ‘C3, 4, 5 keep the diaphragm alive’.
It has an extensive blood supply:
- Arterial supply: the superior surface is supplied by the superior phrenic arteries (from the thoracic aorta), musculophrenic and pericardiacophrenic arteries (from the internal thoracic arteries). The inferior surface is supplied by the inferior phrenic arteries (from the abdominal aorta).
- Venous drainage: the superior surface is drained by the superior phrenic vein, musculophrenic and pericardiacophrenic veins. The inferior surface is drained by the inferior phrenic veins (to IVC and suprarenal vein).
Apertures
The diaphragm has three major apertures:
- Caval hiatus: the inferior vena cava passes through this hiatus, found in the central tendon, at the level of T8. Branches of the right phrenic nerve also pass through this opening.
- Oesophageal hiatus: the oesophagus passes through this hiatus found in the right crus (though left of the midline) of the diaphragm at the level of T10. The vagus nerves and small oesophageal arteries also pass through this hiatus.
- Aortic hiatus: the aorta passes through this hiatus at the level of T12 located between the crus and the vertebral column. The azygous and hemiazygous veins and the thoracic duct also pass through this hiatus.
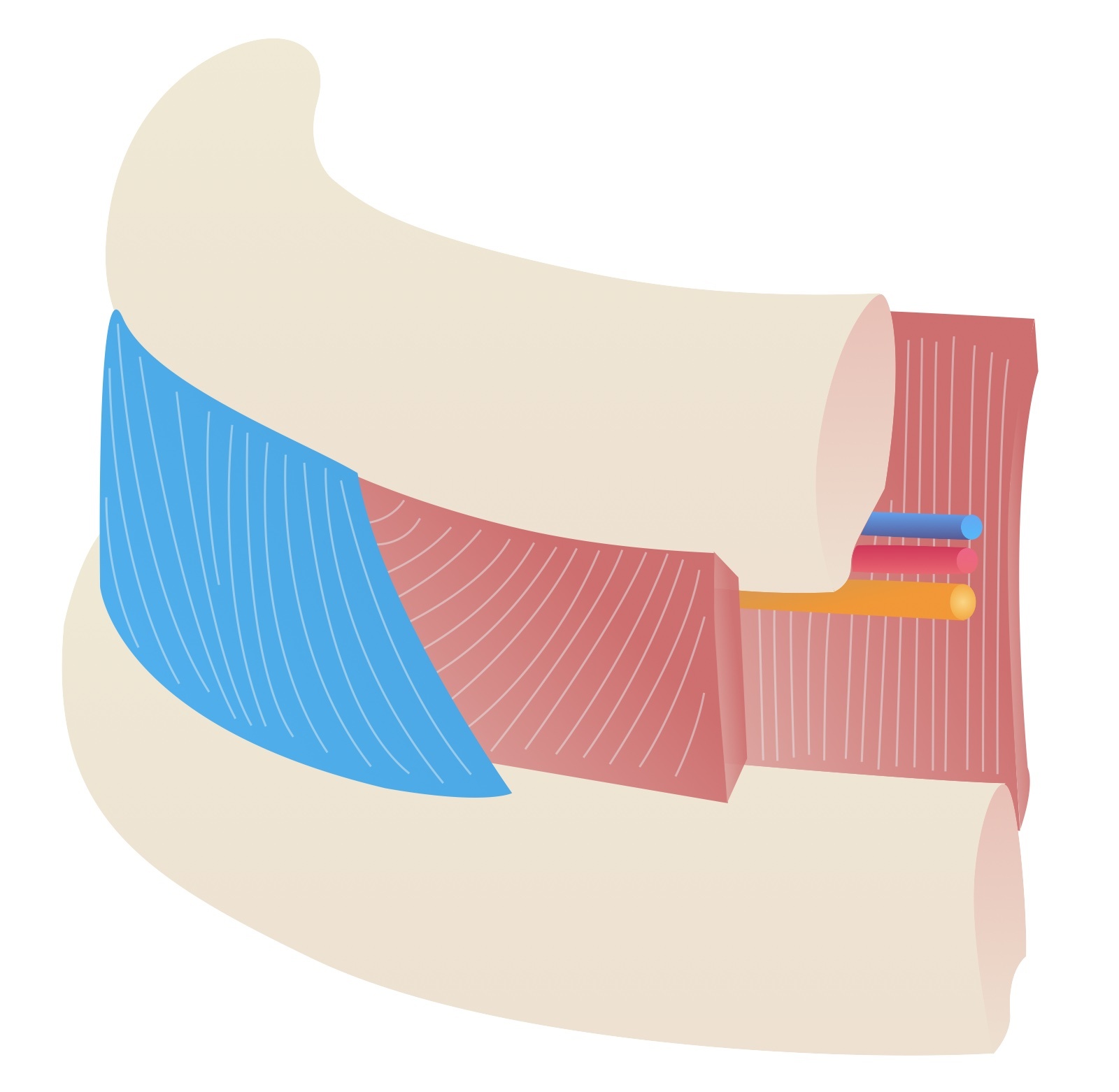
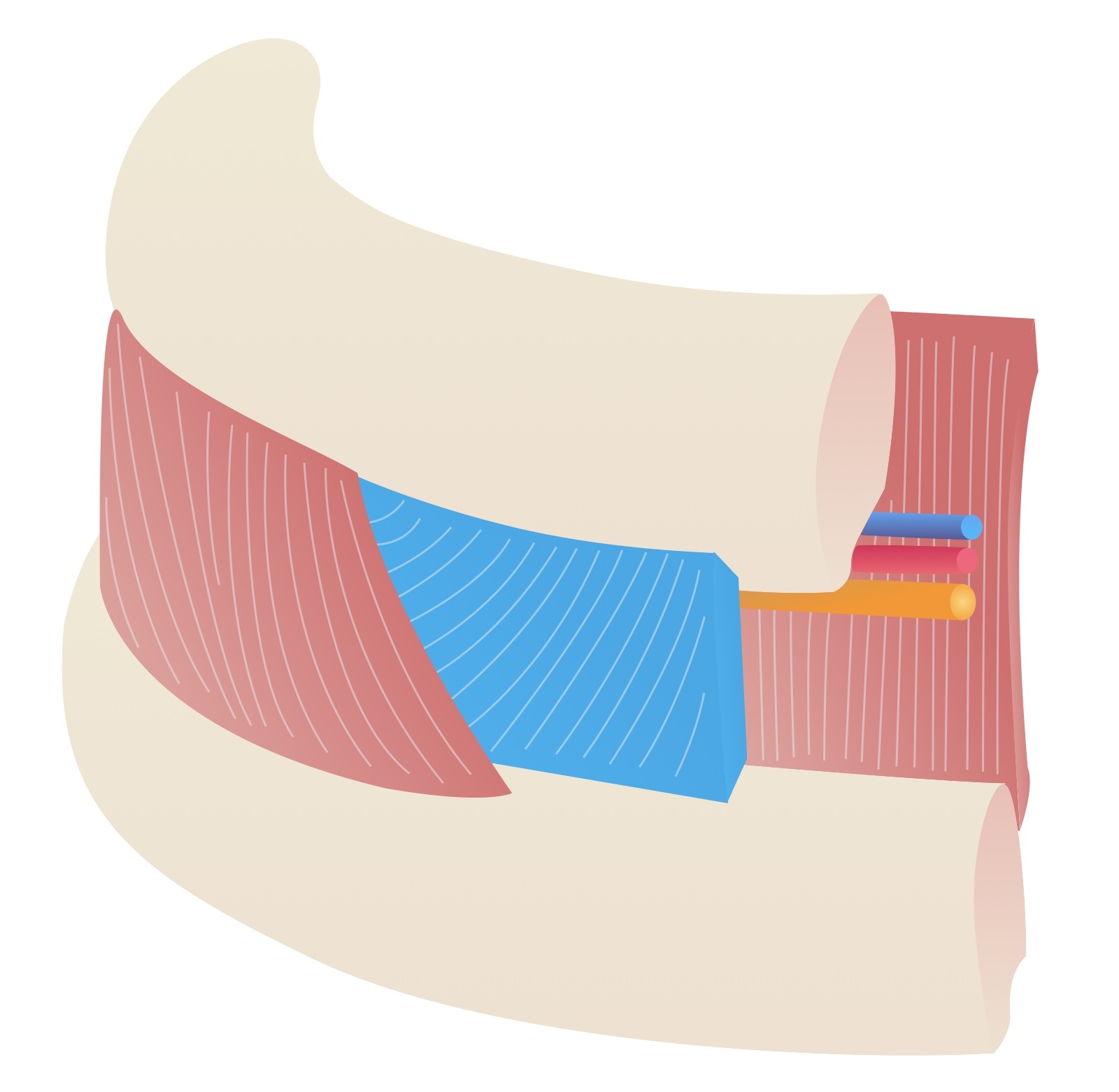
External intercostals
There are 11 pairs of external intercostal muscles whose fibres run inferoanteriorly.
Contraction of these muscles brings the ribcage upward and outward – increasing both the anterior-posterior and lateral diameter of the chest. This expansion of the thoracic cavity causes the inward flow of air.
The muscles run from the costochondral junction anteriorly to the rib tubercles posteriorly. Each muscle originates from the inferior border of the rib above and inserts onto the superior border of the rib below. Anteriorly the muscles blend with the external intercostal membranes which continue to the sternum. Inferiorly they are continuous with the external oblique muscles.
- Arterial supply: intercostal arteries
- Venous drainage: intercostal veins
- Nervous supply: intercostal nerves
Accessory muscles
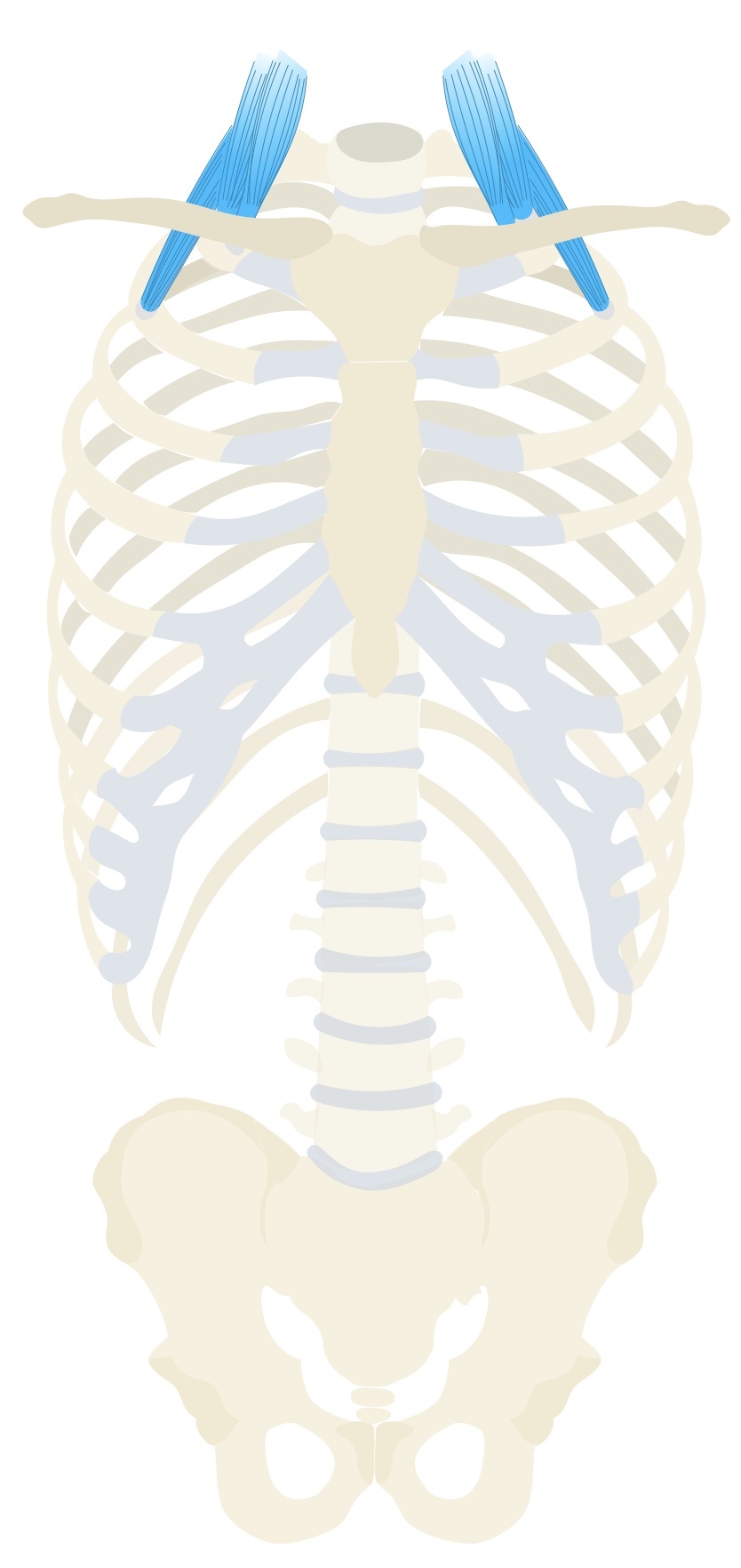
Sternocleidomastoid
The sternocleidomastoid (SCM) is a strap-like muscle that acts to rotate and flex the neck. It is innervated by the accessory nerve.
During forced respiration it may act as an accessory muscle assisting with inspiration. It causes elevation and outward movement of the rib cage.
The SCM inserts superiorly at the mastoid process. Inferiorly, it has two heads with separate origins. The heads are separated by the lesser supraclavicular fossa:
- Sternal head: manubrium
- Clavicular head: medial third of the clavicle.
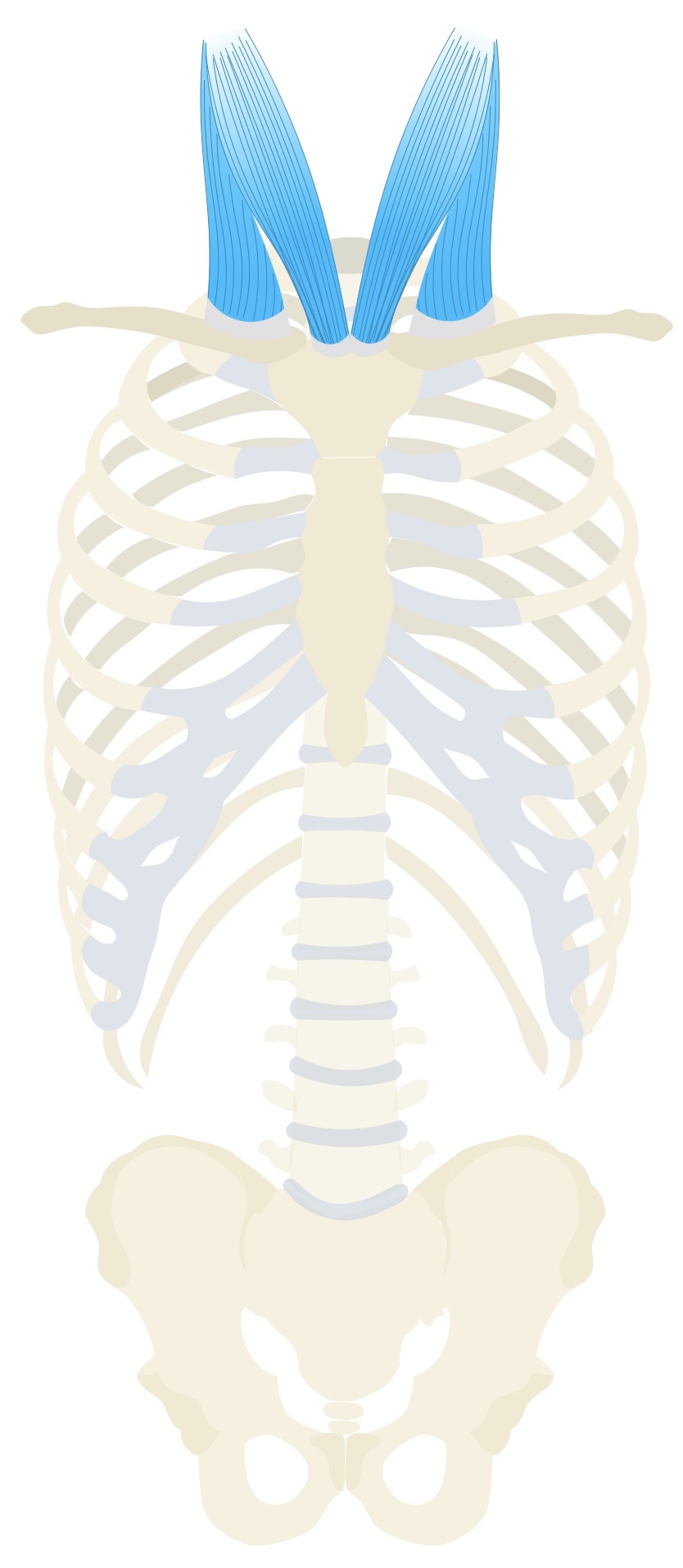
Scalenes
The scalenes are a trio of prevertebral muscles capable of flexing the neck.
During forced inspiration they act as an accessory muscle and are capable of elevating the upper two ribs.
Anterior scalene
- Superior origin: C3-C6
- Inferior insertion: 1st rib
Middle scalene
- Superior origin: C5-C7
- Inferior insertion: 1st rib
Posterior scalene
- Superior origin: C5-C7
- Inferior insertion: 2nd rib
Expiration
Normal expiration is a passive process that relies on the elastic recoil of the lungs. A number of muscles are recruited for forced expiration.
In quiet expiration the diaphragm relaxes and lung tissue recoils resulting in the expulsion of air. During active or forced expiration a number of muscles may be recruited:
- Internal intercostals (interosseous component)
- Muscles of the abdominal wall
Internal intercostals
There are 11 pairs of internal intercostal muscles whose fibres run inferoposteriorly. They are situated deep to the external intercostal muscles and their fibres run at right angles to each other.
Each muscle originates from the inferior border of the rib above and inserts onto the superior border of the rib below.
- Arterial supply: intercostal arteries
- Venous drainage: intercostal veins
- Nervous supply: intercostal nerves
It is thought that the interosseous component of the internal intercostals act primarily during forced expiration helping to depress the ribs.
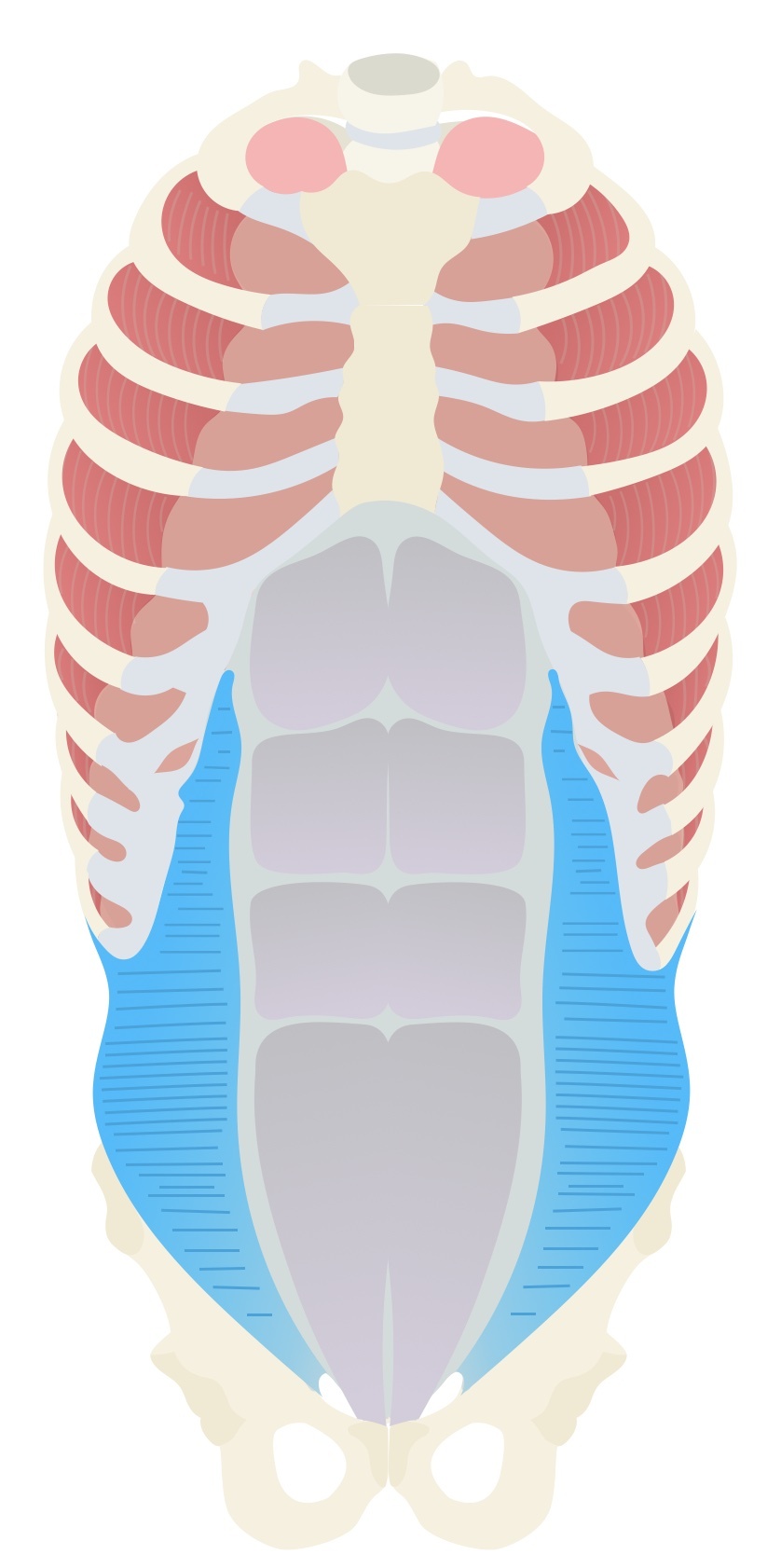
Muscles of the Abdominal wall
Rectus abdominis
The rectus abdominis are paired muscles divided into four sections by tendinous intersections.
- Origin: pubic symphysis, iliac crest.
- Insertion: xiphoid process and costal cartilages of ribs 5-7.
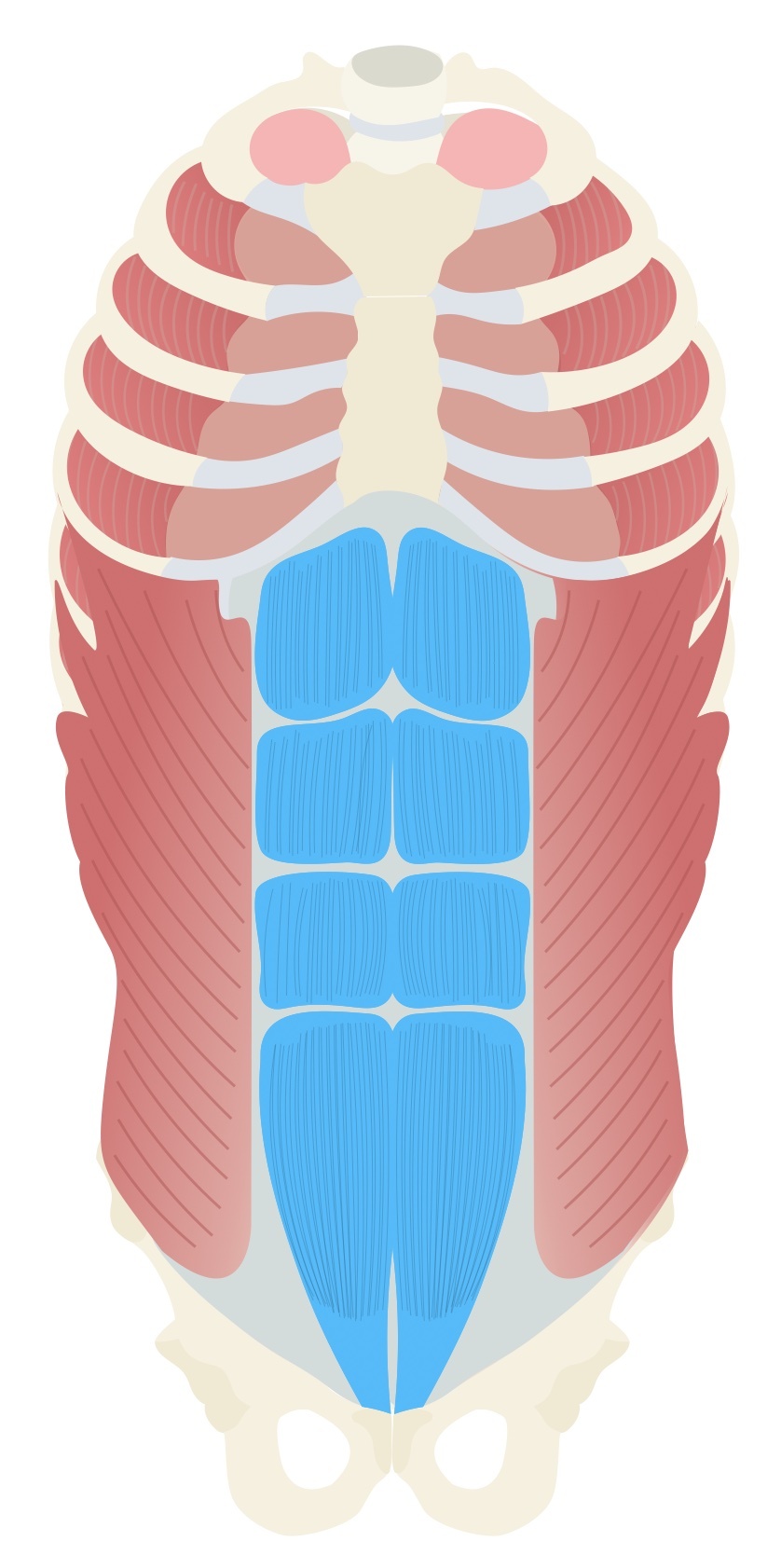
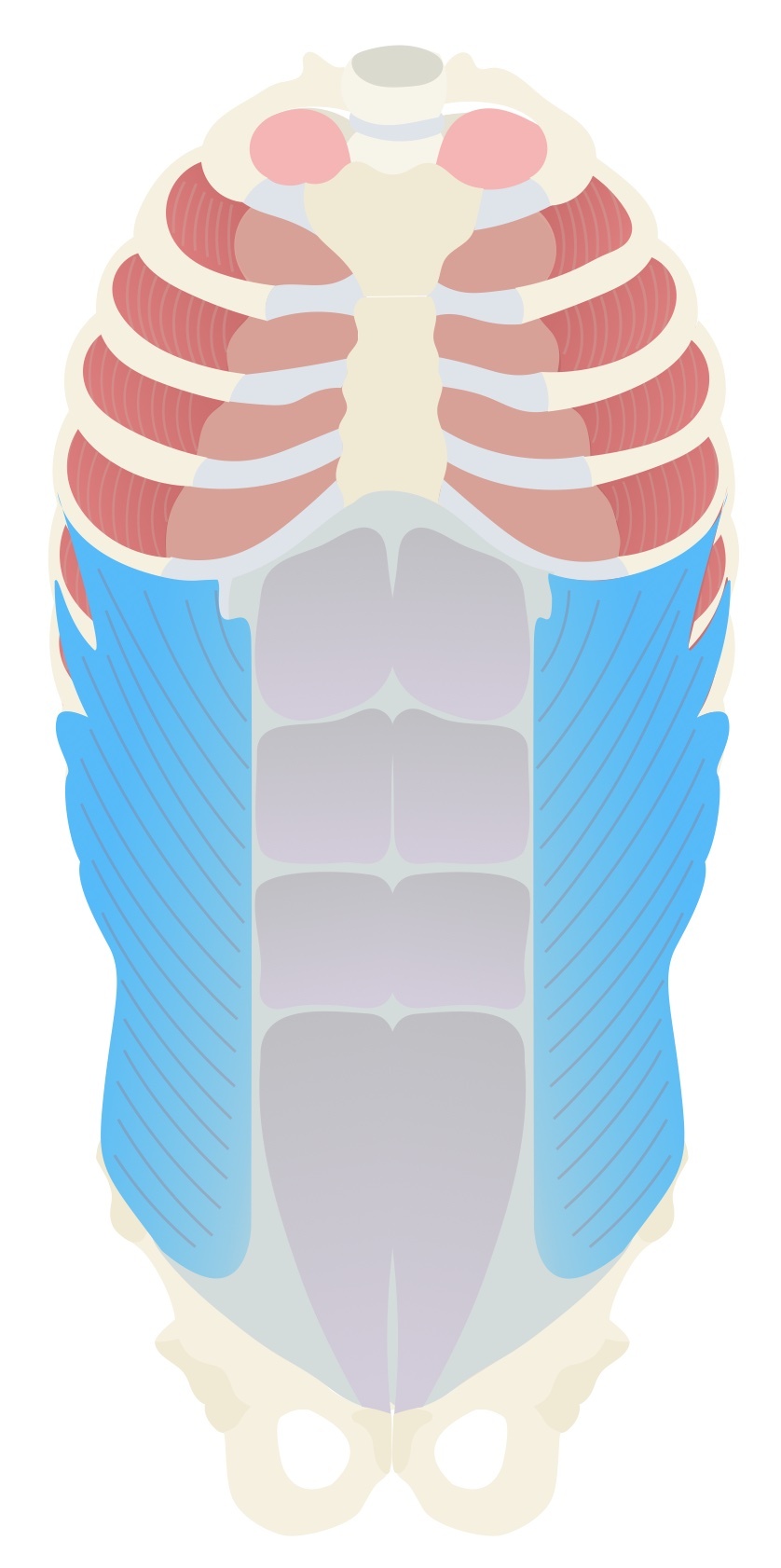
External oblique
The external oblique is the largest of the three anterolateral abdominal muscles whose fibres run inferomedially.
- Origin: external surface of ribs 5-12.
- Insertion: linea alba, pubic tubercle, iliac crest.
A central aponeurosis connects the two muscular components. The inferior edge is thickened, running from the anterior superior iliac spine (ASIS) to the pubic tubercle as the inguinal ligament.
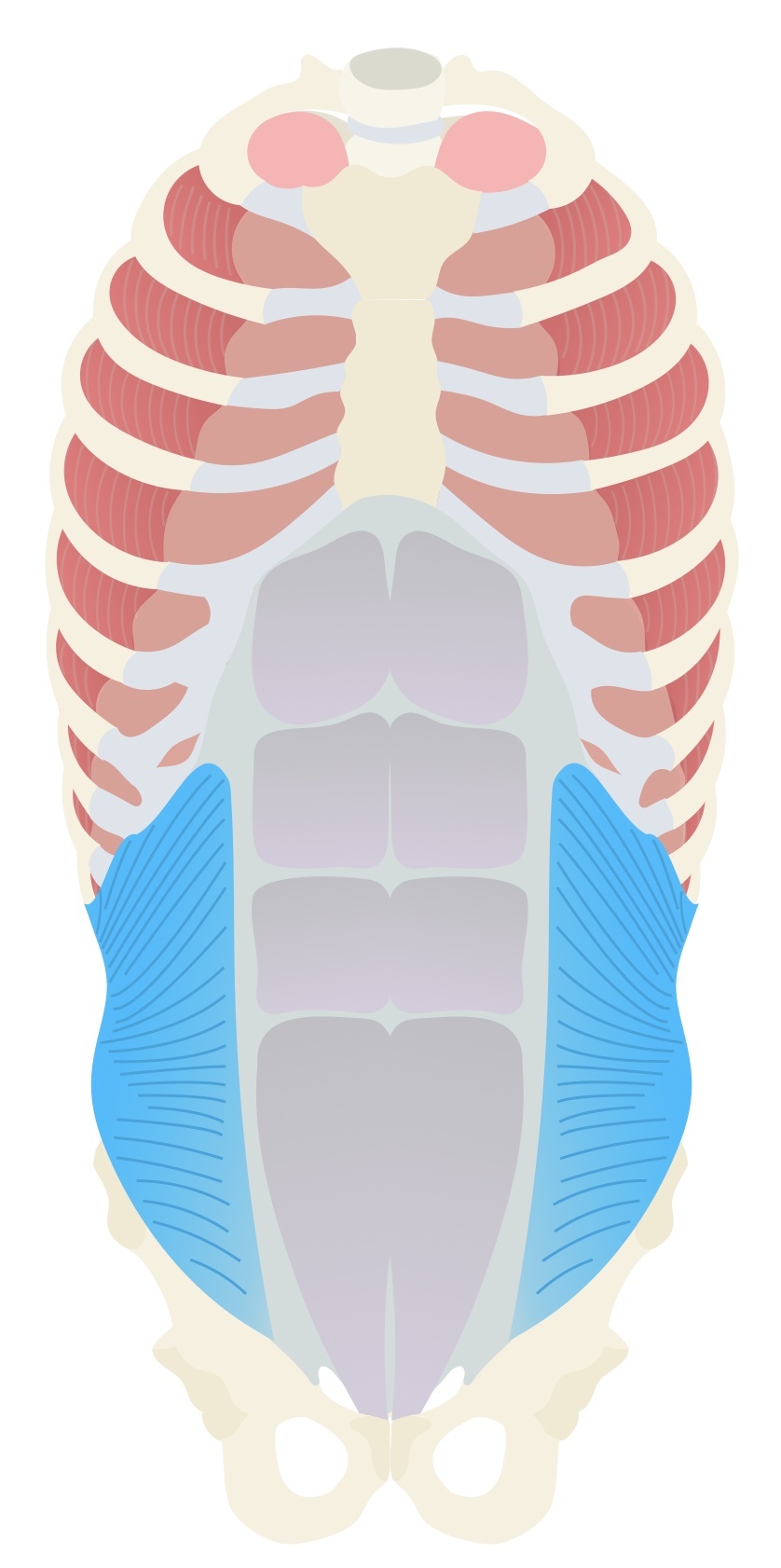
Internal oblique
The internal oblique is the middle of the three anterolateral abdominal muscles whose fibres run superomedially.
- Origin: thoracolumbar fascia, iliac crest.
- Insertion: inferior borders of ribs 10-12, linea alba, pecten pubis.
Transversus abdominis
The transversus abdominis lies deep to the internal oblique and its fibres run transversally across the abdomen.
- Origin: the internal surface of the costal cartilage of ribs 7-12, thoracolumbar fascia, iliac crest.
- Insertion: linea alba, pecten pubis.
Its circumferential nature makes it suited to compressing the contents of the abdominal cavity.