Overview
Non-Hodgkin lymphomas are the sixth most common type of cancer in the UK.
Lymphoma is a haematological malignancy arising from lymphoid tissue. They are commonly categorised as Hodgkin or Non-Hodgkin lymphoma:
- Hodgkin lymphoma (HL): Characterised by the presence of Hodgkin/Reed-Sternberg cells (large, multinucleated cells). Further categorised as classical Hodgkin’s lymphoma (nodular sclerosis, mixed cellularity, lymphocyte-rich and lymphocyte-depleted) and nodular lymphocyte-predominant Hodgkin’s lymphoma.
- Non-Hodgkin lymphoma (NHL): Reed-Sternberg cells are not seen in NHL. There are more than 60 subtypes and they can be B-cell or NK/T-cell in origin. B-cell lymphomas are more common accounting for around 80%, though there is significant geographic variation. NHLs are more common than Hodgkin lymphoma, accounting for around 80-85% of lymphomas.
Epidemiology
There are around 14,000 cases of NHL diagnosed in the UK each year.
In the UK, prevalence increases with age, with most diagnosed after the age of 55 – however it is one of the more common cancers in young people. The 80-84 age-group is most commonly affected.
In 2017, it was the sixth most common cancer in the UK and was responsible for around 4,900 deaths. Overall males are more often affected and there was no significant difference between ethnicities according to figures from Cancer Research UK.
Presentation
The most common symptom of NHL is lymphadenopathy.
Presentation is dependent on the type of NHL and its grade. They may be high-grade and aggressive, presenting with rapidly enlarging masses, malaise, fevers, weight loss and night sweats.
Conversely they may be low-grade, more indolent, with gradual lymphadenopathy, malaise and signs of marrow involvement.
Features common to many NHLs include:
- Lymphadenopathy
- Fever
- Night sweats
- Weight loss (unexplained, > 10% in the last 6 months)
- Pruritus
- Splenomegaly
- Hepatomegaly
Together, weight loss, night sweats and fever are called ‘B’ symptoms.
Each sub-type of NHL has its own pattern of clinical features. Presentations can range from dermatological conditions to bowel obstruction to superior vena cava obstruction.
Some patients will present with primary extra-nodal lymphoma, examples include:
- Primary CNS lymphoma: Neurological features such as headache, confusion, seizures and coma may develop.
- Primary cutaneous lymphoma: Patients may present with rashes, plaques and ulcers. Examples include mycosis fungoides, a cutaneous T-cell lymphoma.
- Primary GI tract lymphoma: Patients may present with abdominal pain, nausea, obstruction and haemorrhage.
Oncological emergencies
On occasion patients with NHL may present with, or develop, an oncological emergency.
These include, but are not limited to:
- Superior vena cava obstruction (SVCO)
- Cord compression
- Hypercalcaemia
- Tumour lysis syndrome
- Neutropenic sepsis
Investigations
Biopsy is normally required for diagnosis, excision biopsy is preferred to core biopsy.
Exact investigations are dependent on the type of NHL, however a biopsy is normally required. Fine needle aspiration is not considered adequate and excisional biopsy (ideally) or core biopsy should be obtained.
Bloods
- FBC
- UE
- LFT
- ESR
- Bone profile
- LDH
- Uric acid
- HIV, Hep B and Hep C
Imaging
- Chest x-ray
- CT neck, chest, abdomen and pelvis: Allows assessment and identification of enlarged lymph nodes, the liver and spleen and soft tissue masses.
- PET CT: Used both in the staging and assessment of treatment response in many lymphomas. Lymphomas are often FDG avid, though some will not be.
- MRI brain: Particularly used when leptomeningeal infiltration or mass lesions are suspected.
- Testicular USS: Identify suspected testicular lymphoma (a rare type of testicular tumour).
- Bone scan
Biopsy
Excision biopsy of affected lymph nodes or tissue is normally required in patients with suspected NHL.
Needle core biopsy may be considered in those unfit for excisional biopsy. However, if this fails to produce a sufficient sample an excisional biopsy will have to be reconsidered.
Additional
- Bone marrow aspirate and biopsy
- Lumbar puncture: In patients with suspected CNS disease, cytology and flow cytometry may be required.
- Fluorescence in situ hybridisation (FISH): NICE advise using FISH to identify MYC rearrangement in those with high-grade B-cell lymphoma. If found, further testing to identify BCL2 and BCL6 rearrangements and the immunoglobulin partner should be arranged.
Lugano staging
The Lugano staging system is used to classify NHL.
It describes the anatomical distribution of disease and is of both prognostic and therapeutic importance.
The system originates from an international conference in Switzerland in 2011 (and many further meetings), and is an attempt to update the Ann-Arbor system to reflect changes in the decades since it was introduced.
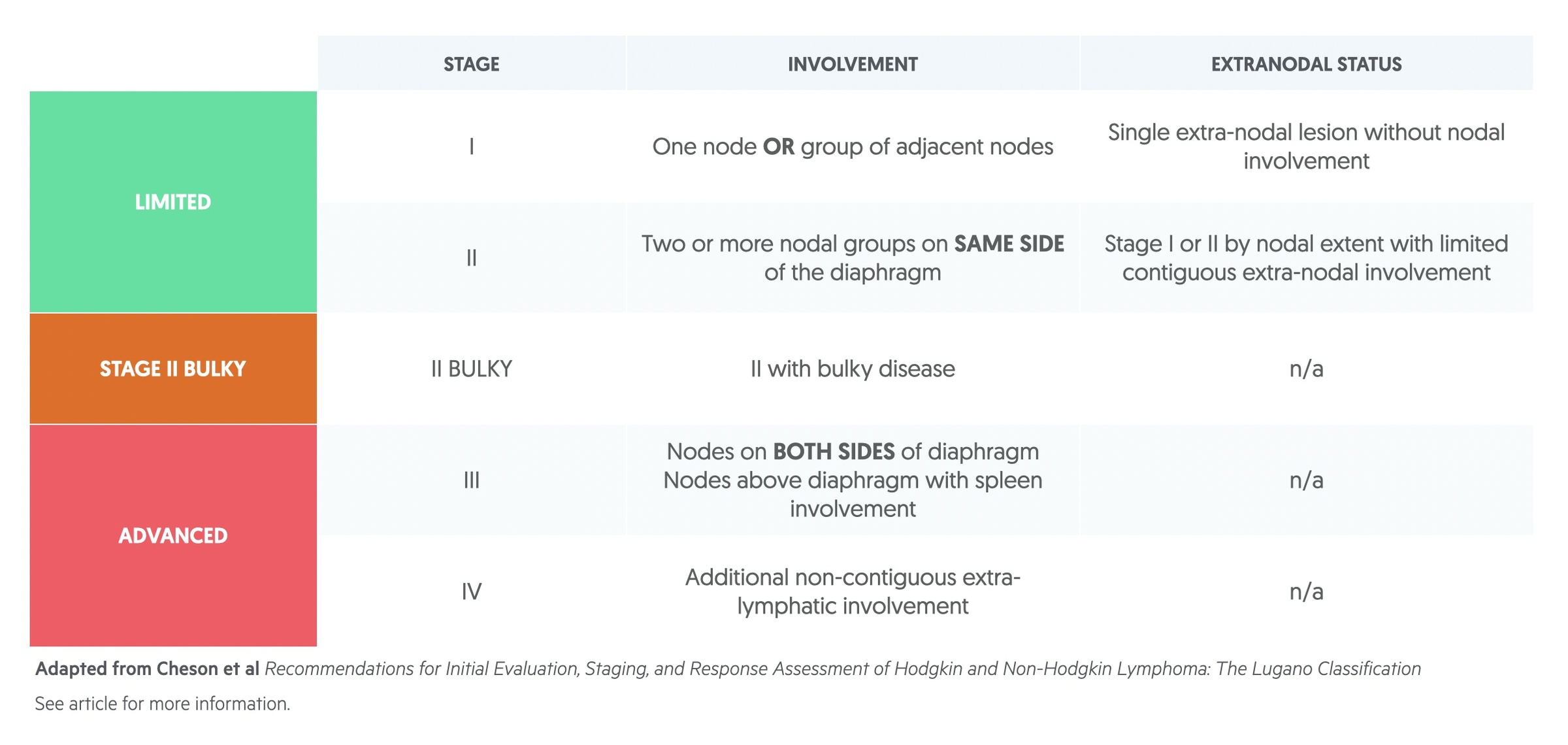
The staging is further modified by the presence or absence of a number of features:
- ‘B’ symptoms: ‘B’ symptoms refer to fever, night sweats and weight loss (unexplained, >10% in 6 months). ’B’ denotes presence and ‘A’ denotes absence.
- Extranodal involvement: In limited stage disease ‘E’ is used to denote extranodal tissue involvement.
- Bulky disease: Definition of bulky is nuanced but typically refers to disease > 10cm.
R-CHOP
R-CHOP is a commonly used chemotherapy regimen in those with NHL.
There are many treatments regimens for NHL. However the one you will be commonly expected to know about at undergraduate level is R-CHOP.
- Rituximab: A monoclonal antibody with activity against CD20 – an antigen found on the surface of B-cells. Serious side effects include infusion reactions, hepatitis B reactivation, mucocutaneous reactions and progressive multifocal leucoencephalopathy.
- Cyclophosphamide: An alkylating agent, inhibits DNA synthesis through cross linking of DNA. It has carcinogenic tendencies and has been linked to the development of a number of malignancies including transitional cell carcinoma of the bladder. Other serious side effects include bone marrow suppression and infertility.
- Doxorubicin: An anthracycline that inhibits topoisomerase II leading to inhibition of DNA and RNA synthesis. Side effects include cardiomyopathy, myelosuppresion and skin reactions.
- Vincristine: Inhibits microtubule formation by binding to tubulin. Side effects include peripheral neuropathy and bladder atony.
- Prednisolone: Is a glucocorticoid steroid. Its side effects are those of steroids.
DLBCL
Diffuse large B cell lymphoma (DLBCL) is the most common form of NHL.
Overview
DLBCL accounts for around 25-30% of all NHL. Within the condition, a number of distinct entities exist and are listed in the WHO classification. It is slightly more common in men than women, and appears to present at a younger age in those of black ethnicity.
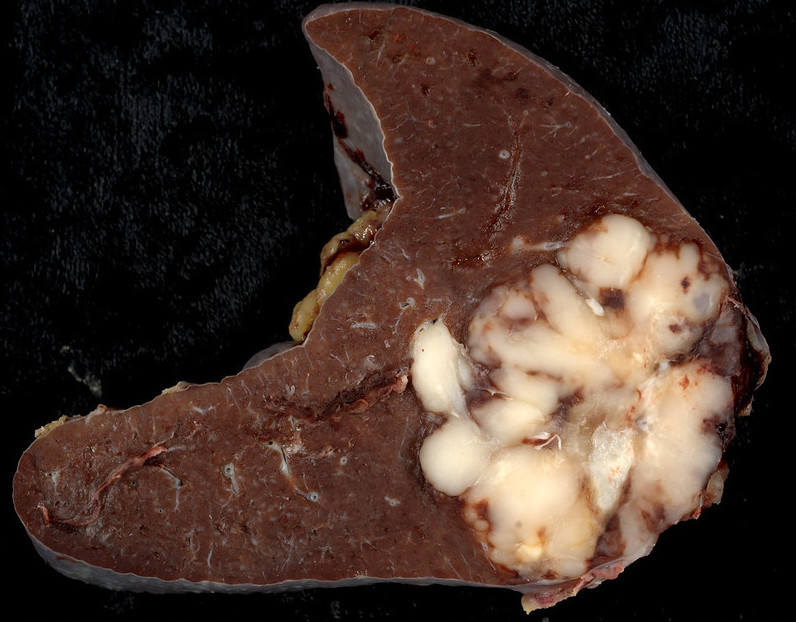
DLBCL involving the spleen
Image courtesy of Dr Ed Uthman
Presentation
Patients tend to present with a rapidly enlarging mass, commonly in the neck, abdomen or mediastinum. ‘B’ symptoms are seen in around a third of patients.
Extranodal disease is common and can arise essentially anywhere but is most commonly seen in the GI tract.
Disease in the mediastinum may lead to SVCO whilst bony destruction may result in a presentation with cord compression.
Treatment
Treatment of DLBCL is enormously complex. Patients will typically be categorised as having limited disease (stage I/II) or advanced disease (stage III/IV). They require assessment for CNS involvement and consideration as to the need for CNS prophylaxis.
- Limited stage disease: Is commonly treated with chemoimmunotherapy in the form of R-CHOP. Combined modality therapy (CMT) may be used where chemoimmunotherapy is combined with radiotherapy.
- Advanced stage disease: Treatment may involve R-CHOP or other regimens such as (da)-EPOCH-R.
Autologous haematopoietic cell transplantation is used at times, typically in the setting of recurrent disease.
Follicular lymphoma
Follicular lymphoma is a B-cell NHL, and the second most common form.
Overview
Follicular lymphoma is the second most common form of NHL. It often presents insidiously, with gradual lymphadenopathy.
The exact pathogenesis is not understood. Around 85% have a translocation between chromosomes 14 and 18, t(14;18), however this is a non-specific change that may be seen in many without lymphoma.
The Follicular Lymphoma International Prognostic Index (FLIPI) is be used to assess prognosis.
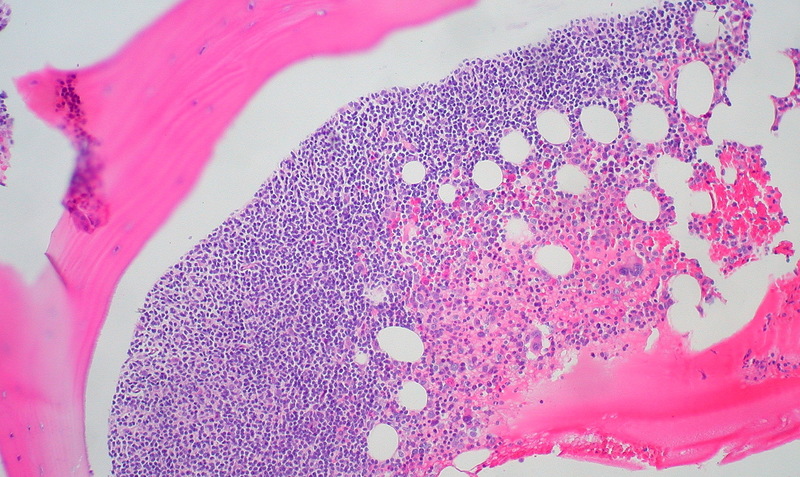
Follicular lymphoma in bone marrow
Image courtesy of Dr Ed Uthman
Presentation
Follicular lymphoma often presents in an insidious manner with gradually worsening, painless lymphadenopathy. The degree of lymphadenopathy may ‘wax and wane’ over time. ’B’ symptoms of weight loss, fever and night sweats are sometimes present.
Treatment
Treatment of follicular lymphoma depends on the stage at diagnosis. For disease caught in the earlier stages (Stage I / II) local radiotherapy may be offered. In those with Stage II disease, or higher grade disease, treatment may more mirror that described for advanced stage disease. ’Watch and wait’ can be used in those in whom radiotherapy is unsuitable.
Cure is not common in those with stage II, III and IV disease and relapse is frequently seen. In patients with stage III/IV disease (advanced disease) and some with stage II, treatment depends on whether or not they are symptomatic. Treatment may involve immunotherapy with rituximab in those who are asymptomatic. In patients who are symptomatic chemoimmunotherapy is frequently offered with rituximab combined with chemotherapy regimens (e.g CVP, CHOP)
Burkitt’s lymphoma
Burkitt’s is a high-grade, rapidly proliferating, B-cell NHL, that commonly affects children.
Overview
In the UK Burkitt’s is relatively uncommon, with around 210 cases each year. It is the most common NHL in children in the UK and it more frequently affects males.
It may be grouped into three types:
- Endemic: Strongly associated with Epstein-Barr virus (EBV), and follows the distribution of malaria. It is often seen in equatorial Africa.
- Sporadic: Less commonly associated with EBV, often seen in Europe and North America.
- Immunodeficiency: Associated with AIDs or in other conditions / medications that lead to immunosuppression.
It is caused by mutation to c-myc proto-oncogene. This most commonly occurs due to a translocation between chromosomes 8 and 14, t(8;14)(q24;q32).
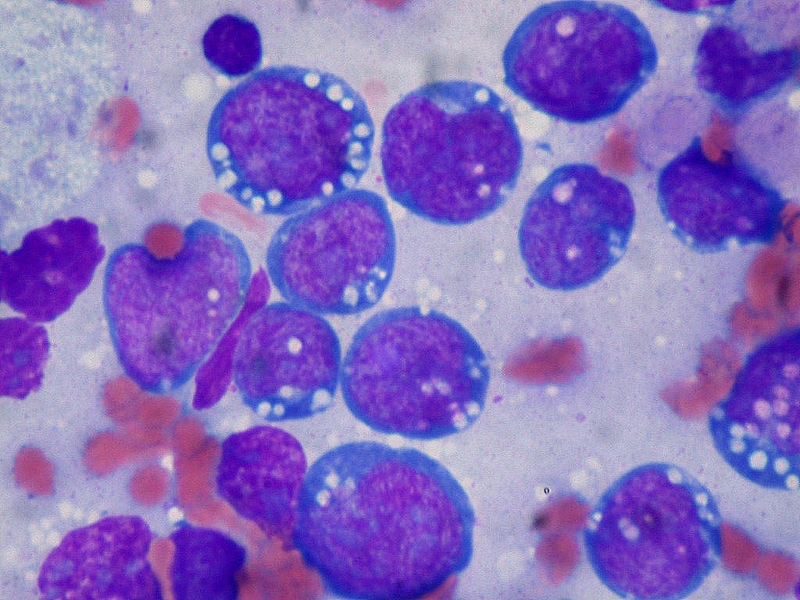
Burkitts lymphoma, touch prep, Wright stain
Image courtesy of Dr Ed Uthman
Presentation
Endemic Burkitt’s classically presents with a rapidly enlarging tumour in the jaw of a child. It can also present with enlarged lymph nodes in the neck and abdominal masses.
Sporadic Burkitt’s more commonly presents with abdominal symptoms, with the ileoceacal valve often affected. It may present with bowel obstruction.
Fever, weight loss and night sweats may all be present.
Management
As with all areas of NHL, treatment is complex and depends on the patients health, wishes and disease type. As with most high-grade lymphomas it is highly chemosensitive.
First line treatment frequently involves intensive immunochemotherapy, options include:
- R-BFM
- R-CODOX-M/R-IVAC
- R-HyperCVAD (HDMTX)
- R-LMB
Less intensive immunochemotherapy options are available for those not suitable for more intense options, including R-CHOP, R-CHEOP and DA-EPOCH-R.
In those with lower risk disease DA-EPOCH-R regimen may be used with methotrexate (intravenous and/or intrathecal).
Due to rapid tumour breakdown on the initiation of treatment the risk of tumour lysis syndrome is high and prophylactic treatment is normally required.

