Introduction
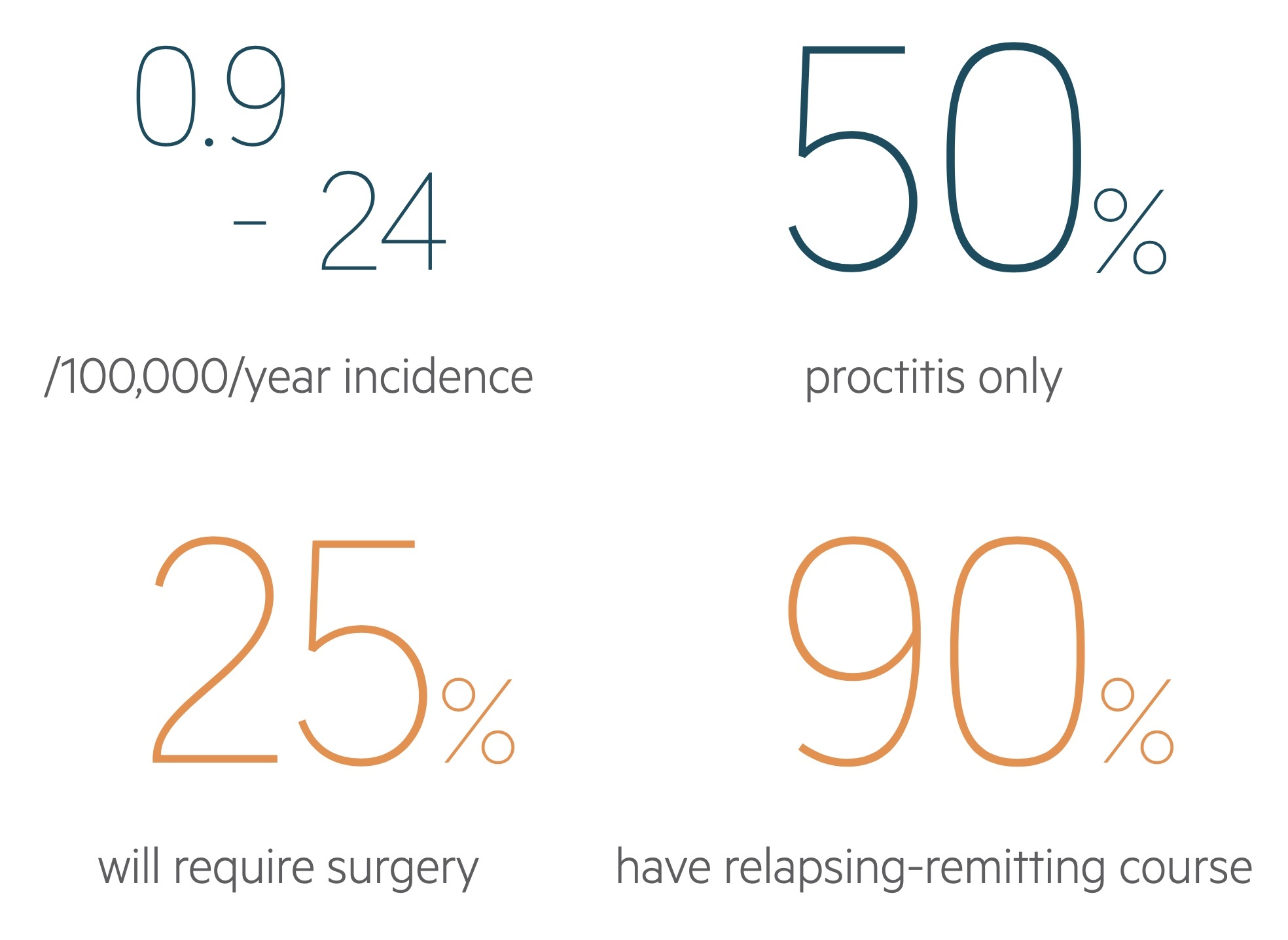
Ulcerative colitis is a chronic, inflammatory disease characterised by a relapsing-remitting course affecting the gastrointestinal tract.
Inflammatory bowel disease
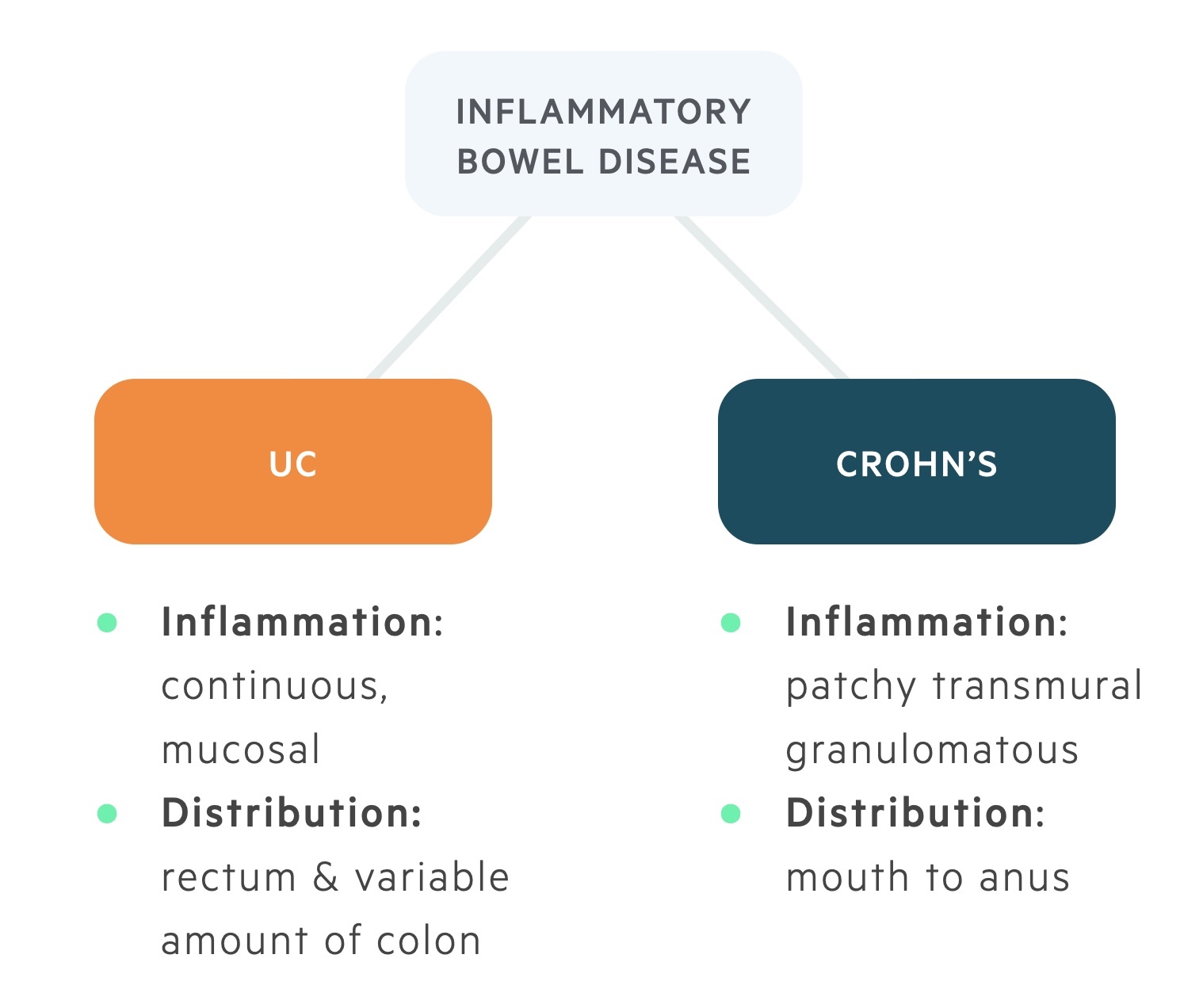
Inflammatory bowel disease (IBD) is an umbrella term for two chronic inflammatory disorders of the gastrointestinal system:
- Ulcerative colitis (UC)
- Crohn’s disease (CD)
Though related, the two conditions have different pathologies, presentations and treatments. Whilst UC is a continuous inflammation of the mucosa starting in the rectum (in most cases) and limited to the colon, in CD transmural patchy inflammation is seen throughout the gastrointestinal tract.
Ulcerative colitis
UC is a disease of the colonic mucosa, which has a relapsing-remitting course. It is characterised by inflammation of the mucosa, affecting the rectum (rectal sparing occurs but is rare) and may progress proximally through the colon. The terminal ileum may be affected (‘backwash ileitis’) in those with extensive colitis.
UC is the most common form of IBD, with an estimated prevalence of 240 per 100,000 population. UC is more common in females. There is a bimodal peak in incidence between 15-25 and 55-65 years of age.
Aetiology
The precise aetiology of both UC and CD remains unknown.
The current theory is of an abnormal immunological response and/or increased reaction to commensal bacteria within a genetically susceptible individual. This theory is based around three core aetiological factors: immunity, genetics and the environment.

1. Immunity
There is suggested to be an abnormal immunological response to intestinal microflora. There also seems to be a protective role in patients who have previously had an appendicectomy.
2. Genetics
Ulcerative colitis is a polygenic disease (multiple susceptible genetic loci increase the likelihood of developing UC, but do not directly cause it). It is more common in certain populations (e.g. Jewish) and there is often a positive family history.
3. Environmental
Smoking is protective in UC, whereas it is positively associated with CD. Numerous environmental factors are linked with UC; which include milk consumption, bacterial microflora alteration and medications (e.g. NSAIDs, OCP).
Pathophysiology
A number of pathophysiological changes occur due to inflammation of the colonic mucosa.
Overview
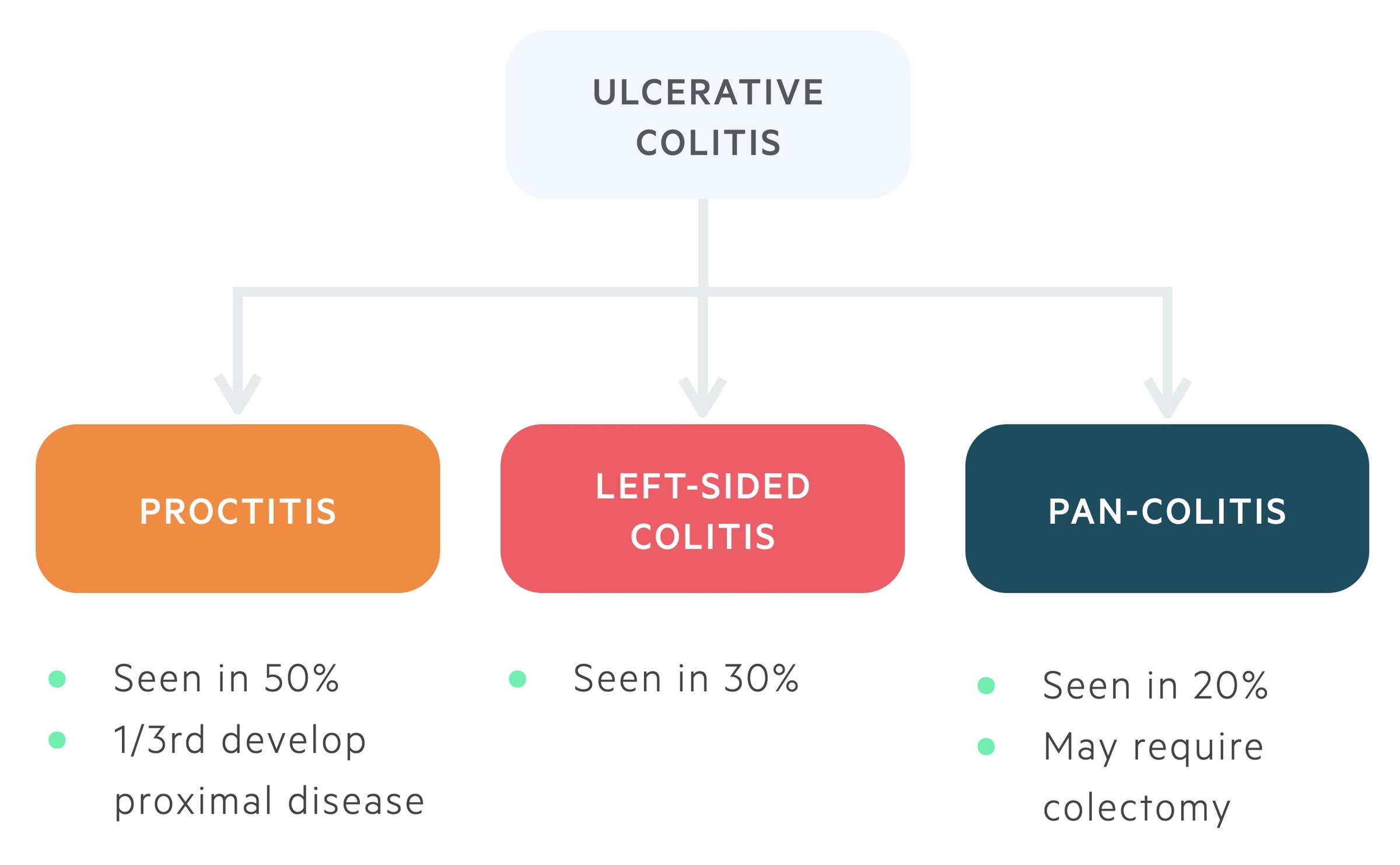
UC affects the rectum (proctitis) first and then extends proximally to involve more of the colon. The extent to which UC affects the colonic mucosa is variable among patients.
Most patients (50%) suffer from proctitis only, however, 1/3rd of these patients will go on to develop more proximal disease. Approximately 30% have left-sided disease and up to 20% have pancolitis.
Pancolitis refers to inflammation of the entire colon. Patients with pancolitis are at risk of developing backwash ileitis. This refers to reflux of colonic contents into the distal few centimetres of the ileum through the ileocaecal valve. Backwash ileitis can make distinction between UC and CD more difficult.
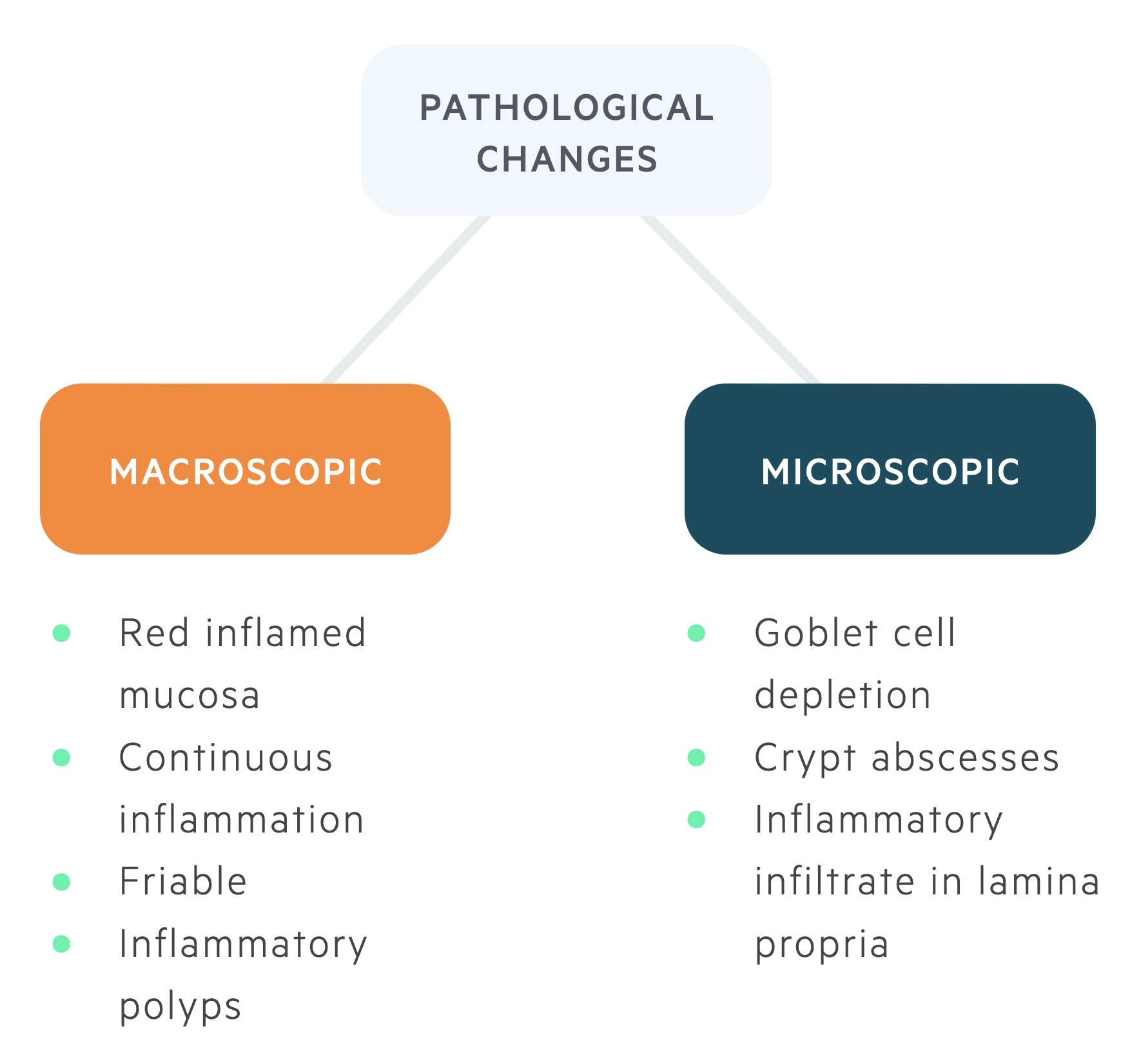
The changes that occur in UC can be described as macroscopic, which are seen during endoscopy or microscopic that are seen on histology.
Macroscopic
Macroscopically there is evidence of continuous inflammation that extends proximally along the colon. The surface of the mucosa appears reddened and inflamed. The mucosa is also said to be easily friable to touch, and there may also be evidence of inflammatory polyps.
Microscopic
Microscopic changes seen in UC are predominantly alterations in crypt architecture with the development of crypt abscesses and goblet cell depletion. There is also increased inflammatory infiltration into the lamina propria, which is largely neutrophilic.
Clinical features
The hallmark of UC is bloody diarrhoea / rectal bleeding.
Patients with UC may become acutely unwell with features of hypovolaemic shock, so it is important to resuscitate patients with respect to airway, breathing and circulation.
Symptoms
- Weight loss
- Fatigue
- Abdominal pain
- Loose stools
- Rectal bleeding
- Tenesmus (incomplete emptying)
- Urgency
Signs
- Febrile
- Pale
- Dehydrated
- Abdominal tenderness
- Abdominal distension/mass
- Tachycardic, hypotensive

Toxic megacolon
A major complication of UC is toxic mega colon (TMC).
TMC is a medical emergency, which refers to toxic, non-obstructive, dilatation of the colon (> 6cm). Patients with UC who present with abdominal distension and tenderness should be admitted for suspected TMC.
Other features suggestive of TMC include systemic symptoms such as:
- Fever
- Tachycardia
- Hypotension
- Dehydration
- Altered mental status
- Biochemical abnormalities (e.g. leukocytosis, anaemia, and electrolyte derangements)
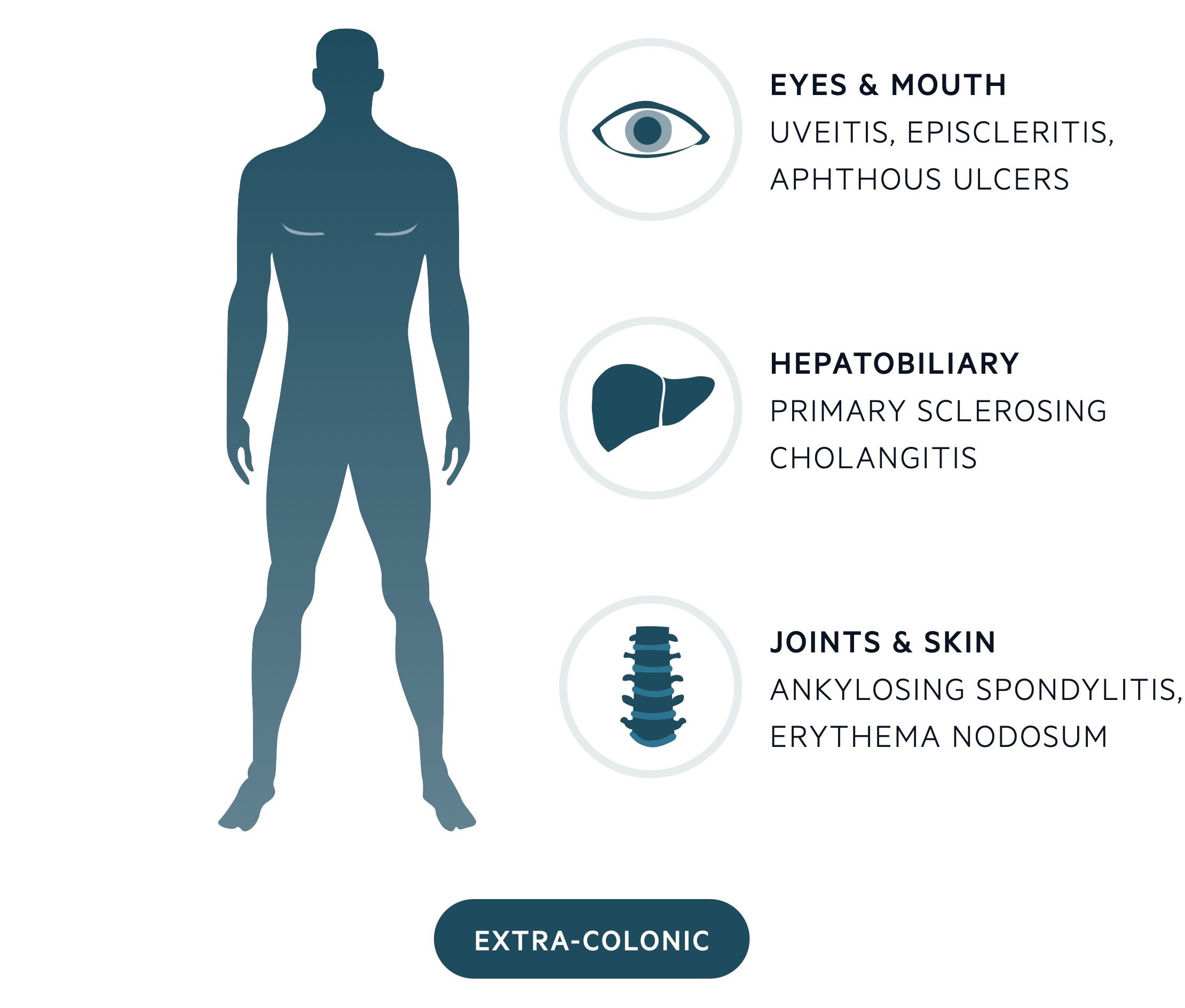
Extra-colonic manifestations
Approximately 25% of patients will develop extra-colonic manifestations during their lifetime.
Musculoskeletal
Arthritis is the most common extracolonic manifestation, which may be a simple peripheral arthritis or more complex spondyloarthropathy (e.g. ankylosing spondylitis). Other important musculoskeletal features include osteopaenia/osteoporosis and the presence of clubbing of the hands and feet.
Eyes, mouth & skin
Uveitis (inflammation of the uvea) is strongly associated with UC. Uveitis may be divided into anterior, intermediate and posterior. Other ophthalmic features include episcleritis, which refers to superficial inflammation of the sclera.
Extracolonic manifestations of the mouth commonly include aphthous ulcers. The skin is another organ widely affected by UC, leading to erythema nodosum, which is a type of panniculitis that classically results in multiple, painful, purple nodules on the anterior aspect of the shins.
Hepatobiliary
Numerous hepatobiliary pathologies are associated with UC including fatty liver disease and autoimmune liver disease.
However, the most common pathology is primary sclerosing cholangitis (PSC). PSC is thought to affect 3% of patients suffering from UC. Importantly, 70-95% of patients with PSC have UC. PSC should be suspected in any UC patient who has an isolated rise in ALP.
Haematological
Two common haematological problems associated with UC are anaemia and thromboembolism. Both should be considered in any patient presenting with an acute exacerbation of UC, as they may require additional medical intervention.
Investigations & diagnosis
Diagnosis is based on macroscopic assessment (e.g. endoscopy) and histological evidence (e.g. biopsy) of colonic inflammation.
Bedside
- Observations
- ECG
- Urinalysis
- Stool microscopy, culture & sensitivities
- Ova, cysts and parasites
- C. diff toxin (CDT)
- Faecal calprotectin (marker of intestinal inflammation)
Bloods
- Full blood count
- Liver function tests
- Urea & electrolytes
- CRP
- Arterial/venous blood gas
- Haematinics
- Magnesium
- Clotting
- Autoantibodies (e.g. p-ANCA)
Imaging
Abdominal X-rays are useful for looking at dilatation of the bowel and perforations. Dilatation is said to be present if:
- Small bowel: diameter > 3cm
- Large bowel: diameter > 6cm
- Caecum: diameter > 9cm
Computed tomography may be organised where there is concern regarding complications (e.g. toxic megacolon) and prior to surgery.
Endoscopy
Colonoscopy is considered the diagnostic investigation of choice as it allows assessment of the whole colon. Biopsies can be taken for histological assessment of the mucosa. Caution should be taken during acute flares due to the increased risk of perforation. Sigmoidoscopy may be used as an alternative endoscopic test.
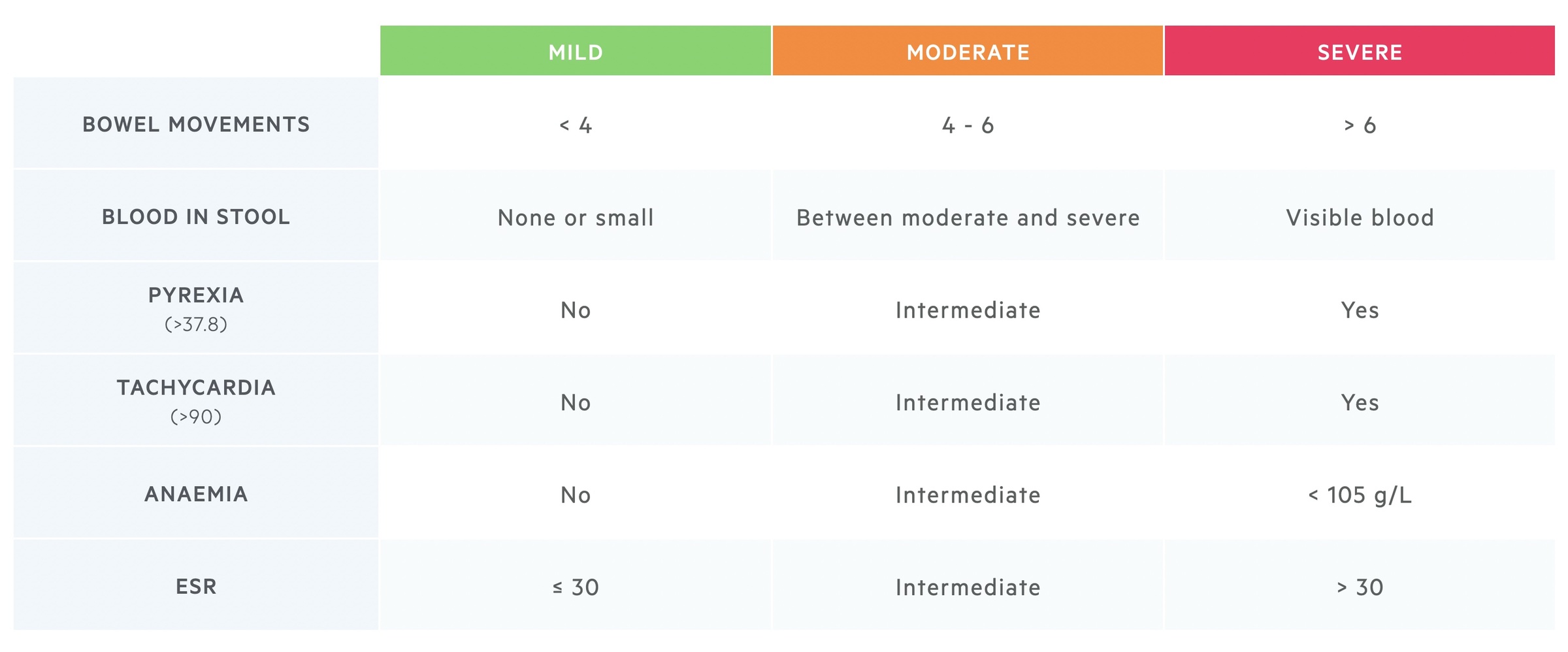
Truelove & Witts
The severity of UC in adult patients can be assessed using the Truelove & Witts’ classification.
The Truelove and Witts’ scoring categorise the severity of acute presentations of UC into mild, moderate and severe. You will notice a degree of variation (and modifications) in re-productions of this score, primarily a reflection of the relatively vague definition of moderate (or ‘moderately severe’) in the original paper.
Mild
- < 4 bowel motions per day.
- Small amount of blood.
Moderate
- 4-6 bowel motions per day.
- Quantity of blood between mild and severe.
Severe
- > 6 bowel motions per day.
- Visible blood
- Systemic upset
NOTE: The Paediatric Ulcerative Colitis Activity Index (PUCAI) is used in paediatric patients.
Management
The general principle in the management of UC is to induce and then maintain remission.
In modern medicine, there are numerous pharmacological options for the management of UC, which include steroids, immunosuppressive agents and biologics. These have revolutionised the treatment of UC and prevent many patients from having to undergo total colectomy (complete removal of the colon). Despite success with medications, an estimated 1 in 5 patients with UC have severe symptoms that do not respond to medications and requires surgery.
The choice of therapy will depend on disease severity, location, co-morbidities, patient preference and side-effects. Many patients require different medications during their disease course.
Induce remission
In patients presenting with UC for the first time, or those who develop a flare of UC, the principal aim is to induce remission with aminosalicylates (5-ASA) and/or steroids. In those presenting with acute severe ulcerative colitis based on Truelove & Witts criteria there is a distinct treatment pathway (discussed below).
In patients with mild-to-moderate UC, treatment is initially with 5-ASA agents (topically +/- orally). These medications can be used for both the induction of remission and continued maintenance. Patients with extensive UC (e.g. pancolitis or left-sided colitis) should be treated with both oral and topical (e.g. enemas) 5-ASAs. Those with proctitis (i.e. < 20 cm on flexible sigmoidoscopy) can be treated with 5-ASA suppositories alone.
Patients who fail to respond to maximum dose of 5-ASA agents, or those with moderate-to-severe UC, can be treated with the addition of systemic corticosteroids as a 6-8 week weaning course. Steroid enemas can also be added. If patients do not respond to steroids over a two week course then hospital admission and biologics can be considered.
Maintenance therapy
Pharmacological options to maintain remission in UC predominantly include thiopurines and biologics. These are considered in patients who fail to respond to remission therapy (e.g. steroid-refractory), those who have two or more flares within a 12 month period or those who are steroid-dependent.
- Thiopurines (azathioprine and mercaptopurine): work through purine synthesis inhibition in lymphocytes leading to immunosuppression. Must check TPMT enzyme activity before use. Homozygous mutations in TPMT can lead to dangerous bone marrow suppression. Major side-effects include pancreatitis and hepatotoxicity.
- Biologics: refers to monoclonal antibodies. Options include infliximab/adalimumab (tumour necrosis factor alpha inhibitors), vedolizumab (alpha-4/beta-7 integrin inhibitor) and tofacitinib (JAK inhibitor). More biologic agents are being tested in clinical trials.
Surgical intervention
The principle surgical option in UC is proctocolectomy followed by ileal pouch anal anastomosis (IPAA) or end ileostomy. Surgery may be indicated in patients with acute severe ulcerative colitis that has failed to respond to medical therapy, patients who develop complications (e.g. malignancy, perforation), or those with chronic active symptoms despite optimal medical therapy.
Surveillance colonoscopy
Patients with UC and Crohn’s disease are at increased risk of colorectal cancer. Currently, patients with IBD in the UK are offered surveillance colonoscopy between 6-10 years following diagnosis to screen for dysplasia (abnormal cell growth, predisposes to malignancy). The frequency of surveillance endoscopy depends on the presence of dysplasia, extent of disease, disease activity and co-morbidities. Patients with primary sclerosing cholangitis (PSC) are at a particularly high risk of cancer.
Acute severe ulcerative colitis
Acute severe ulcerative colitis (ASUC) is a life-threatening condition, which requires high-dose intravenous steroids.
Patients with new suspected UC, or those presenting with a flare of UC, need assessment according to Truelove & Witts criteria. Any patients with severe symptoms need admission to hospital for urgent assessment and treatment.
Initial assessment
All patients with suspected ASUC require:
- Inpatient admission
- Bloods: FBC, CRP, U&E, LFT, Mg +/- early pre-biologic screening. Biologic screening refers to a series of blood tests that are needed to ensure it is safe to give a monoclonal antibody that suppresses the immune system.
- Faeces cultures: stool MC&S, OCP (ova, cysts and parasites), C. diff toxin, Stool virology (e.g. norovirus).
- Imaging: abdominal x-ray or computed tomography
- Inpatient lower GI endoscopy: sigmoidoscopy to assess disease activity
Initial treatment
Once confirmed, or highly suspected clinically, patients require treatment with high-dose corticosteroids (e.g. IV hydrocortisone 100 mg QDS) with gastric protection (e.g. proton pump inhibitor).
Other things to consider include:
- Venous thromboembolism (VTE) prophylaxis: patients high risk of VTE (e.g. deep vein thrombosis), so use of low molecular weight heparin (LMWH) is mandatory unless contraindicated (bloody diarrhoea is not a contraindication).
- Antibiotic: any concern about infection should warrant treatment with concurrent broad-spectrum antibiotics
- Hydration and nutrition: patients are high-risk of significant dehydration and poor nutrition. Intravenous fluids, dietitian review +/- nutritional supplements are essential.
Rescue therapy
If patients fail to respond to treatment with 72 hours then rescue therapy should be considered.
Options include:
- Ciclosporin: calcineurin inhibitor. Important in T lymphocyte functioning. Generally given intravenously and levels need to be monitored. If patients have previously been on thiopurines, unlikely to work.
- Infliximab: monoclonal antibody, which targets TNF-alpha. Given as an induction dose and then repeat doses. Can be combined with thiopurines. Main contraindications include latent TB, demyelination and active sepsis.
- Surgical intervention: should be considered in any patient not responding to medical therapy within seven days or development of complications (e.g. toxic mega colon, perforation). Early surgical referral and assessment is critical

