Overview
This is a four-part series covering gastrointestinal physiology.
- Part I – Overview of the gastrointestinal system & the oral cavity.
- Part II – Digestion: stomach & control of digestion.
- Part III – Secretion: pancreas & hepatobiliary system.
- Part IV – Absorption: small intestines.
The gastrointestinal (GI) system can be divided into the digestive tract & accessory organs.
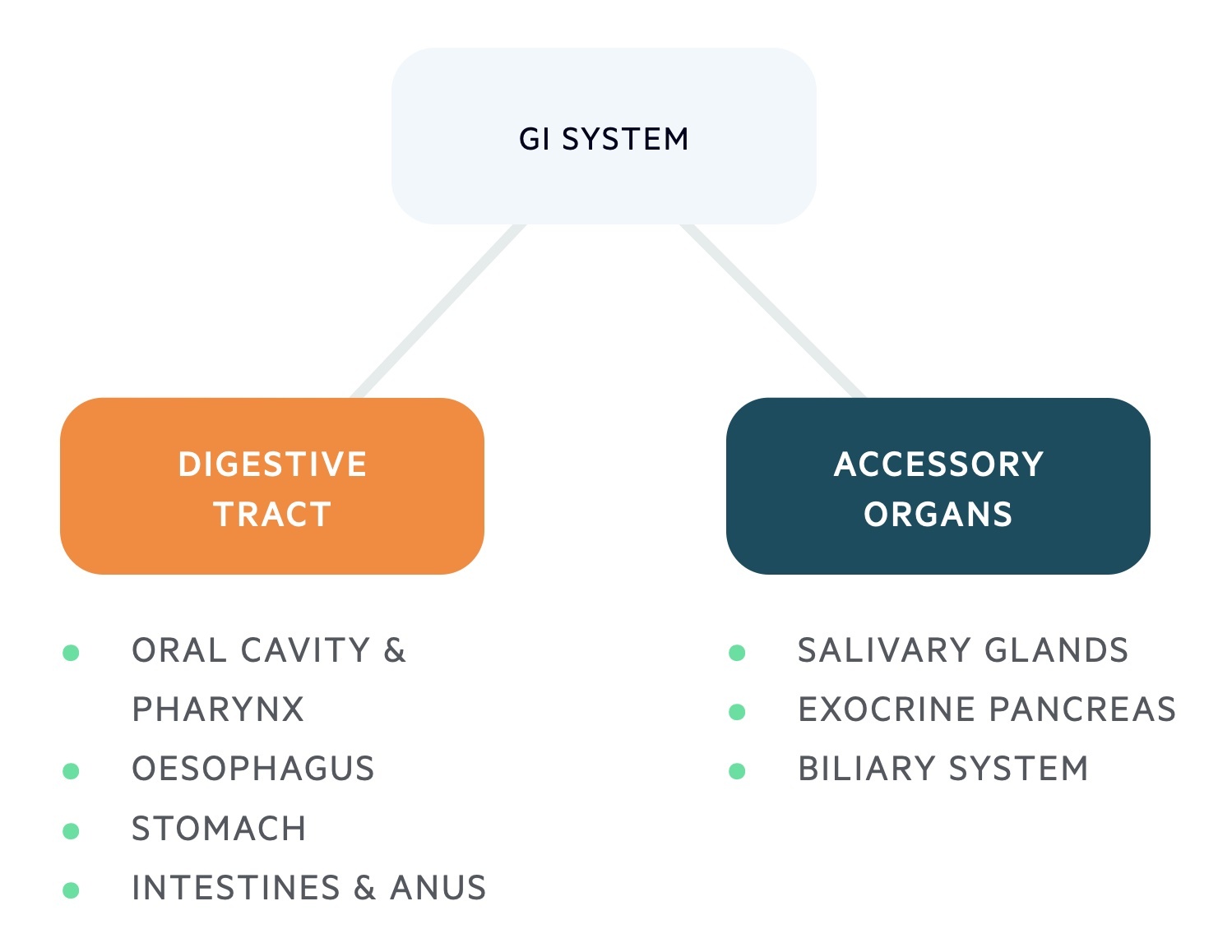
Digestive tract
The digestive tract is a continuous tube that runs from mouth to anus. The lumen of the digestive tract is continuous with the external environment and is therefore not sterile. The digestive tract is approximately 9m in length in its uncontracted state (4.5m in contracted state).
It is divided into different sections:
- Oral cavity
- Pharynx
- Oesophagus
- Stomach
- Small intestines
- Large intestines
- Anus
Accessory digestive organs
There are a number of important exocrine organs which secrete a variety of substances. These substances aid the functions of the digestive tract.
These organs include the three major salivary glands (sublingual, submental and parotid) and the hepatobiliary system (liver, gallbladder and pancreas).
GI tract anatomy
The digestive system tract is divided into several layers: mucosa, submucosa, muscularis externa and serosa.
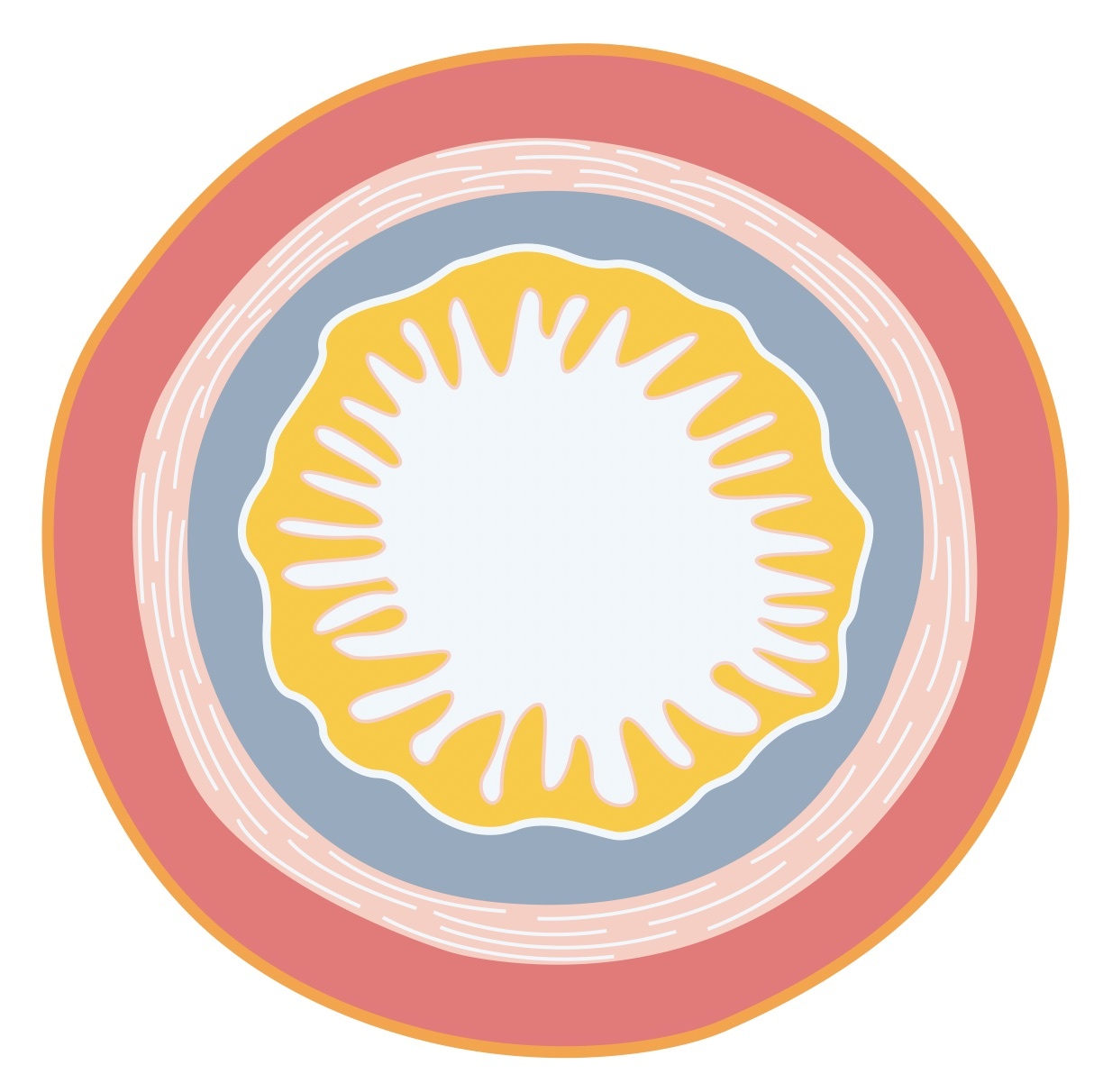
1. Mucosa
The mucosa constitutes the inner lining of the digestive tract. Its epithelial surface forms a mucous membrane with the underlying connective tissue. Collectively, the mucosa is divided into three layers:
- Epithelium
- Lamina propria
- Muscularis mucosa
Epithelium
The epithelium comes into direct contact with the contents of our diet; it forms an important barrier and absorptive surface for all nutrients. It contains numerous exocrine and endocrine cells important in the secretion of enzymes, hormones and digestive juices.
The epithelial lining is specialised to different areas of the digestive tract. The simple columnar epithelium of the stomach is specialised for the harsh, acidic environment. In contrast, the intestinal enterocytes (also columnar epithelium) are specialised for absorption.
Lamina propria
The lamina propria is a layer of connective tissue that sits immediately beneath the epithelium. It contains numerous aggregations of lymphoid tissue called Peyer’s patches, part of the gut-associated lymphoid tissue (GALT). The mucosal-immune interface is an important part of our defence against pathogenic microorganisms.
The lamina propria possesses a rich vascular and lymphatic network that is important for the absorption of nutrients.
Muscularis mucosa
The muscularis mucosa is a thin layer of smooth muscle that sits on the outer surface of the mucosa.
The presence of smooth muscle allows for contraction of this layer. Contraction of the muscularis mucosa results in variation in the folding of the mucosa. This enables exposure of different absorptive surfaces to the luminal contents.
2. Submucosa
The submucosa is a thick layer of connective tissue which provides the GI system with its distensibility and elasticity. The submucosa contains the major blood and lymphatic vessels which supply both the mucosa and muscularis.
The submucosa also contains the submucosal plexus (Meissner’s plexus). This forms part of the enteric nervous system, a branch of the autonomic nervous system.
3. Muscularis externa
The muscularis externa is divided into an inner layer and outer layer of smooth muscle. The inner circular muscle contracts causing narrowing of the lumen. This is important in the mixing of digestive content.
The outer longitudinal muscle shortens the digestive tract, helping to propel digestive contents along its length. Interestingly, the pharynx is the only location where the circular muscle can be found external to the longitudinal muscle (as the superior, middle, and inferior constrictors).
The muscularis externa contains the second neural plexus between its inner and outer layers – called the myenteric plexus (Auerbach’s plexus). Together with the submucosal plexus, it forms the enteric nervous system.
4. Serosa
The serosa is composed of a thin layer of areolar connective tissue with an outer mesothelial layer of simple squamous epithelium.
It forms the outer covering of the digestive tract and is continuous with the visceral peritoneum or mesenteries (double folds of peritoneum).
The serosa secretes a serous fluid to help prevent friction between abdominal viscera.
Functions
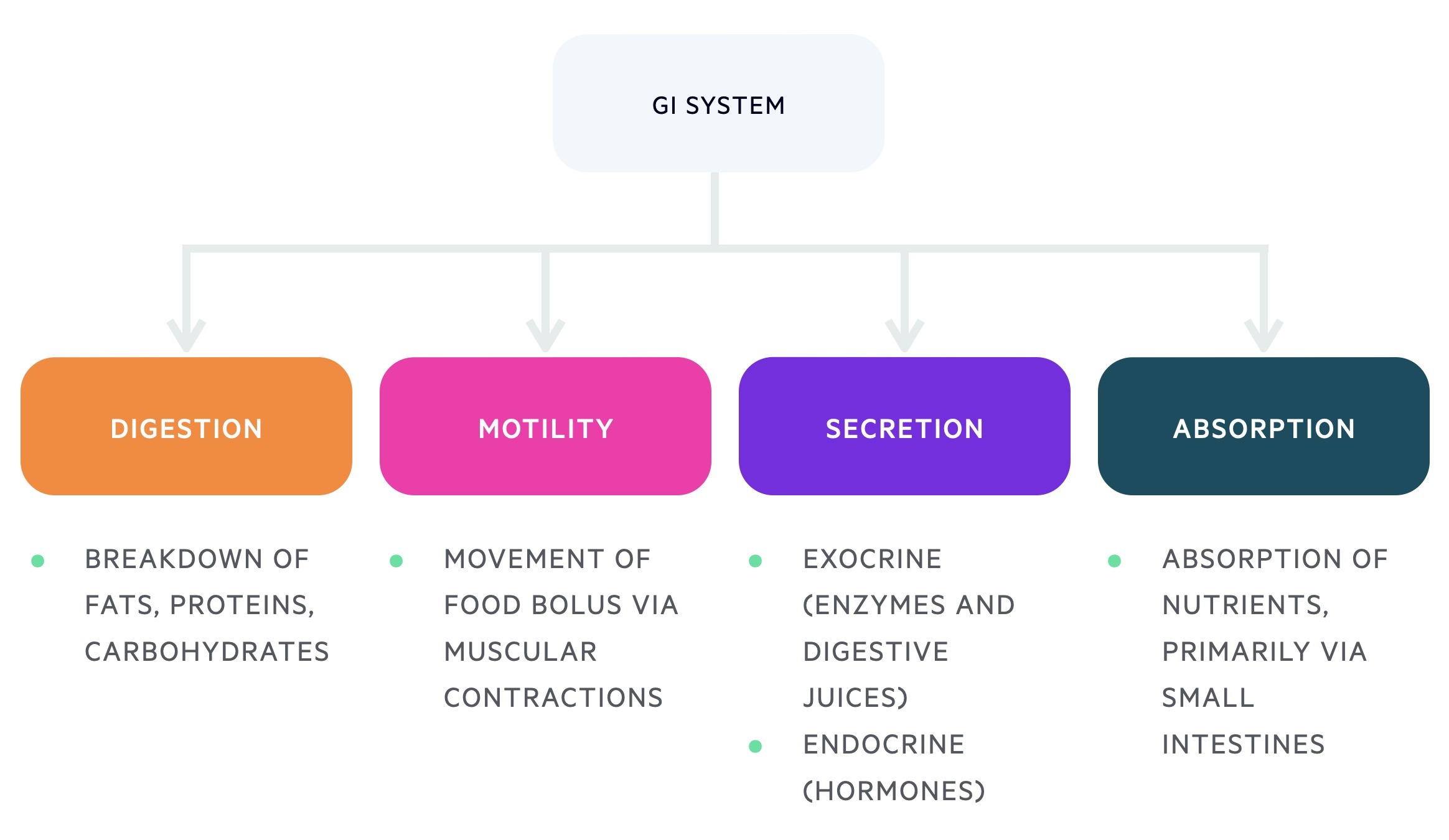
The gastrointestinal tract has four main functions: digestion, motility, secretion & absorption.
1. Digestion
Digestion is the biochemical breakdown of complex molecules (carbohydrates, proteins, lipids) into smaller, absorbable molecules (glucose, amino acids, fatty acids).
Carbohydrates are broken down into disaccharides, and eventually monosaccharides, by the action of different enzymes. Monosaccharides (e.g. glucose, galactose, fructose) can be absorbed by enterocytes and utilised for cellular processes. Proteins, complex structures, are broken down into small peptide fragments and amino acids.
Most dietary lipids are triglycerides. These are broken down into monoglycerides and free fatty acids. Digestion of lipids requires the action of bile. Bile emulsifies large fat globules into smaller ones that pancreatic lipase can act upon.
2. Motility
This is the process of moving food through the digestive tract.
The primary mechanism for movement is peristalsis, which refers to the involuntary contractions and relaxations of the bowel. The peristaltic activity of the digestive tract is under neurohormonal control.
3. Secretion
Both exocrine and endocrine glands are found within the gastrointestinal system:
- Exocrine glands: secrete enzymes and digestive juices that aid in the digestion and absorption of nutrients.
- Endocrine glands: secrete hormones into the blood, which regulate the functioning of the digestive tract.
4. Absorption
The small intestines constitute the primary site of absorption within the GI tract.
The small intestines are well suited for absorption owing to their large surface area and specialised epithelial cells.
Control of the GI system
The functions of the GI tract are controlled by a series of neurohormonal mechanisms.
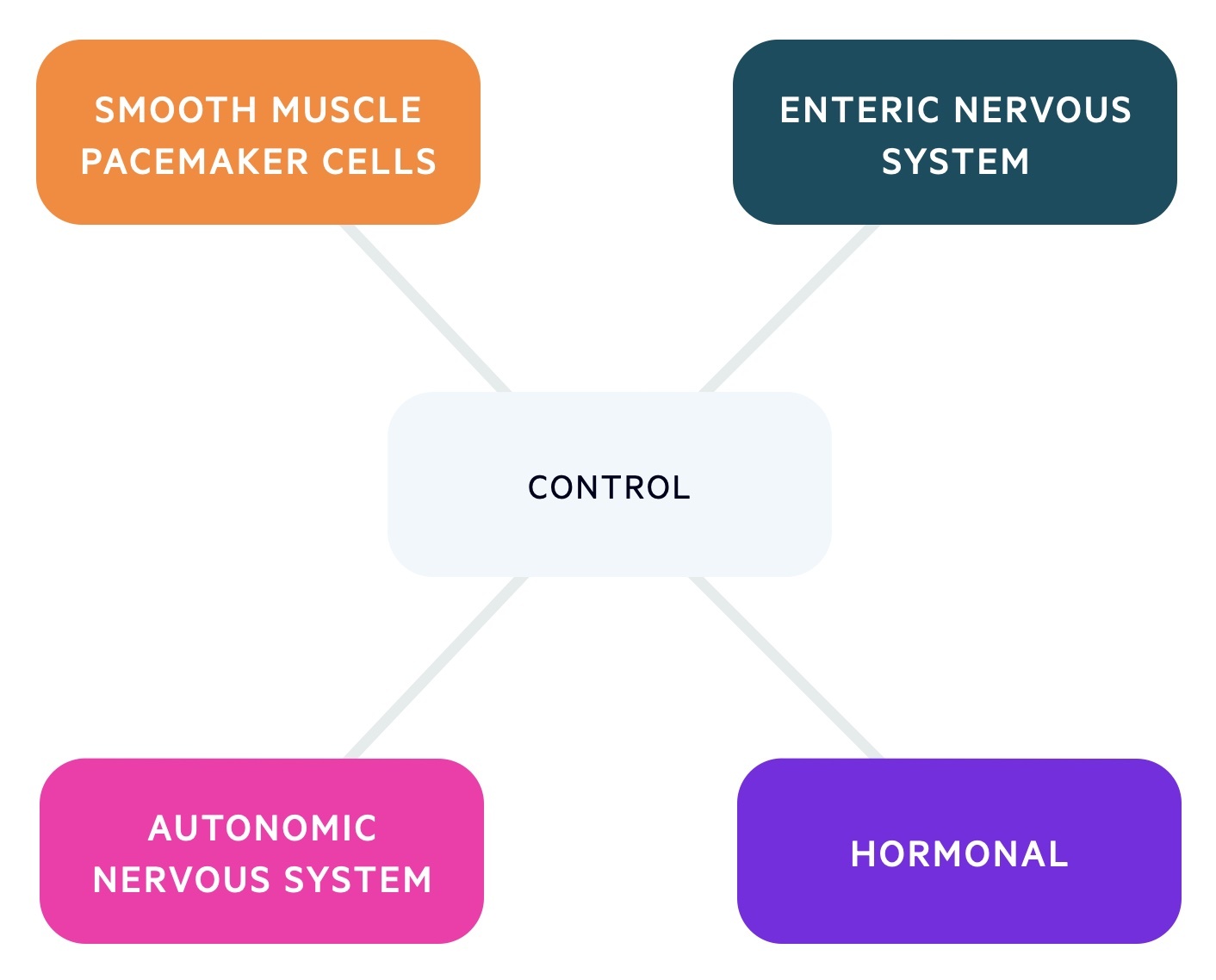
Smooth muscle pacemaker cells
A small number of gastrointestinal cells demonstrate autorhythmicity, similar to cardiac pacemaker cells. These cells are specialised smooth muscle pacemaker cells called the interstitial cells of Cajal (ICC). The ICC can be found within the muscularis externa, between the inner and outer layers. The ICC deliver the electrical activity of the digestive tract, called slow-wave potentials or basic electrical rhythm (BER). The intrinsic rate of slow-wave potentials is set by the ICC and differs depending on the location (e.g. stomach 3/min, ileum 9-10/min).
Slow wave potentials are rhythmic fluctuations in the membrane potential bringing smooth muscle closer (or further away) from threshold potential ( the level at which depolarisation occurs). If the wave reaches threshold potential then a series of action potentials are fired. These cause depolarisation of the sounding muscle fibres and coordinated contraction (via gap junctions).
Enteric nervous system
The digestive tract contains its own intramural nervous system called the enteric nervous system. This is composed of both submucosal and myenteric plexuses. It is considered a subset of the autonomic nervous system containing as many neurones as the spinal cord. Its predominant function is the local control within the digestive tract.
The enteric nervous system contains sensory neurones (which detect local alterations) and effector neurones. The effector neurones are important for muscular contraction, exocrine gland secretion and hormone release.
The importance of the enteric nervous system can be seen in Hirschsprung’s disease. In this condition, there is a congenital absence of submucosal and myenteric plexuses. This leads to an absence of peristalsis, dilatation of the proximal colon and constipation.
Autonomic nervous system
The autonomic nervous system can directly control the digestive tract or modify the effects of the intrinsic nerve plexus and hormonal release. Both arms of the autonomic nervous system (parasympathetic and sympathetic) control the digestive tract.
Parasympathetic activity primarily comes from the vagus nerve. It is involved in the secretion of the neurotransmitter acetylcholine, which binds muscarinic receptors. This increases motility and promotes secretions.
Sympathetic activity arises from the splanchnic nerves. It leads to the release of catecholamines, which predominantly decrease motility and inhibit secretions.
Hormones
Gastrointestinal hormones are secreted into the blood by endocrine glands. Hormones are taken to their site of action where they have stimulatory or inhibitory action on muscular contraction and secretions.
Oral cavity
The oral cavity marks the gateway to the gastrointestinal system.
The oral cavity has a number of important functions. These include: mastication (chewing), sucking, taste, speech and deglutination (swallowing).

Salivary glands
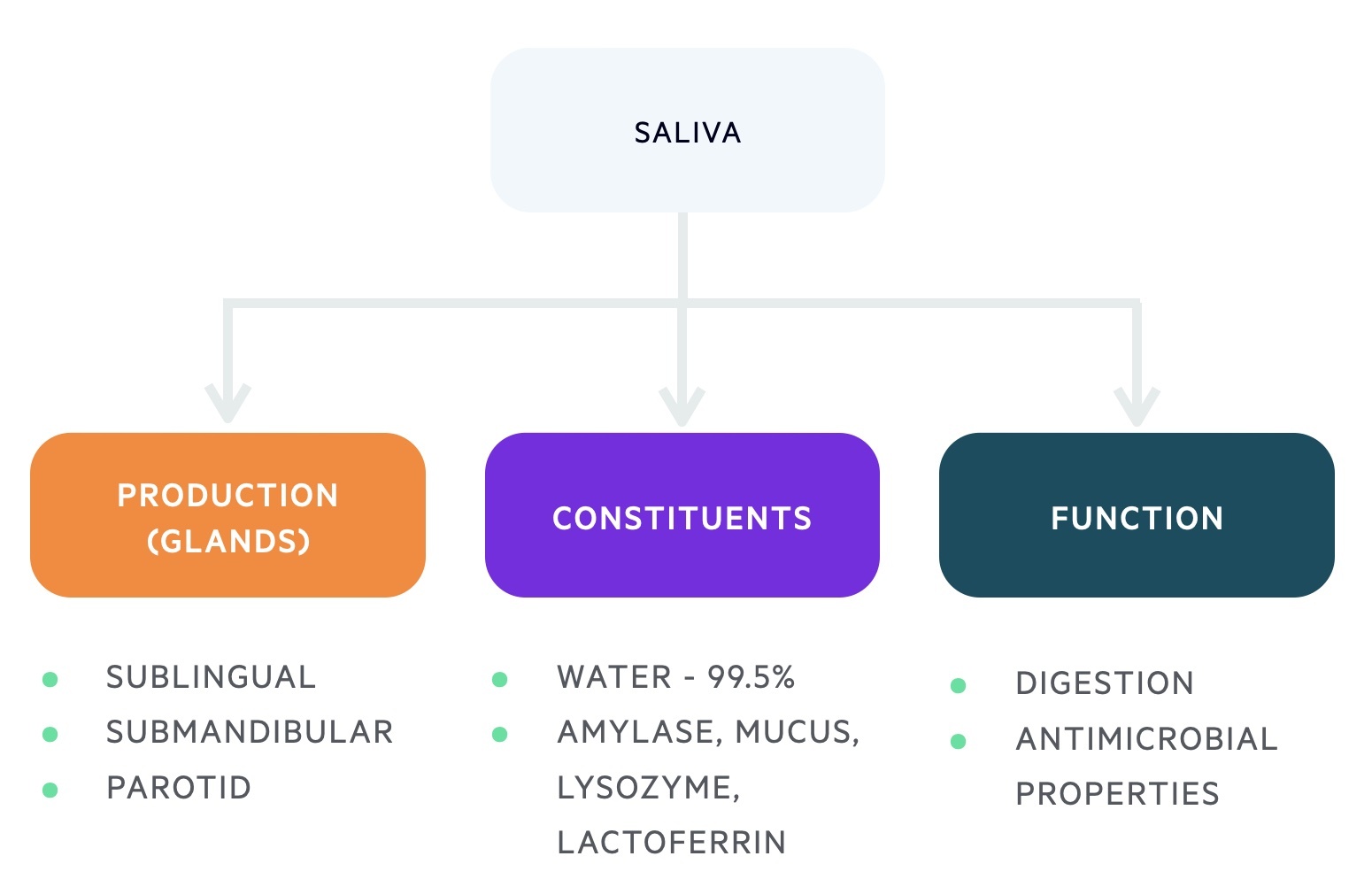
Saliva is produced by the three major salivary glands: sublingual, submandibular and parotid.
Sublingual glands
The sublingual glands, the smallest salivary glands, are situated inferior to the tongue and anterior to the submandibular glands. They are innervated by the facial nerve.
The content of the sublingual glands exits through numerous small ducts in the floor of the mouth.
Submandibular glands
The submandibular glands are situated either side of the floor of the mouth and are innervated by the facial nerve.
The content of these glands passes into Wharton’s duct that exits into the oral cavity either side of the frenulum on the underside of the tongue. Some of the sublingual ducts may join with Wharton’s duct.
Parotid glands
The parotid glands are situated in the pre-auricular area and are innervated by the glossopharyngeal nerve. The facial nerve runs through the parotid gland and divides into its five main branches (temporal, zygomatic, buccal, mandibular, cervical).
The content of the parotid glands exits into the oral cavity via Stensen’s duct at the 2nd superior molar.
Saliva
Approximately 1-2 litres of salvia is secreted each day at a rate between 0.5-5 ml/min. Saliva is an important component of the oral cavity. It has roles in secretion, digestion, taste, speech, hygiene and innate immunity.
The constituents of saliva include water (99.5%), electrolytes, protein (0.5%) as well as:
- Salivary amylase
- Mucus
- Lysozyme (antimicrobial)
- Lactoferrin (binds iron)
Sjögren’s syndrome is an autoimmune condition that leads to the destruction of certain exocrine glands (e.g. salivary and lacrimal). It results in xerostomia (dryness of the mouth). Xerostomia can lead to a number of complications including dysphagia, speech difficulty, dental caries, and difficulty in mastication.
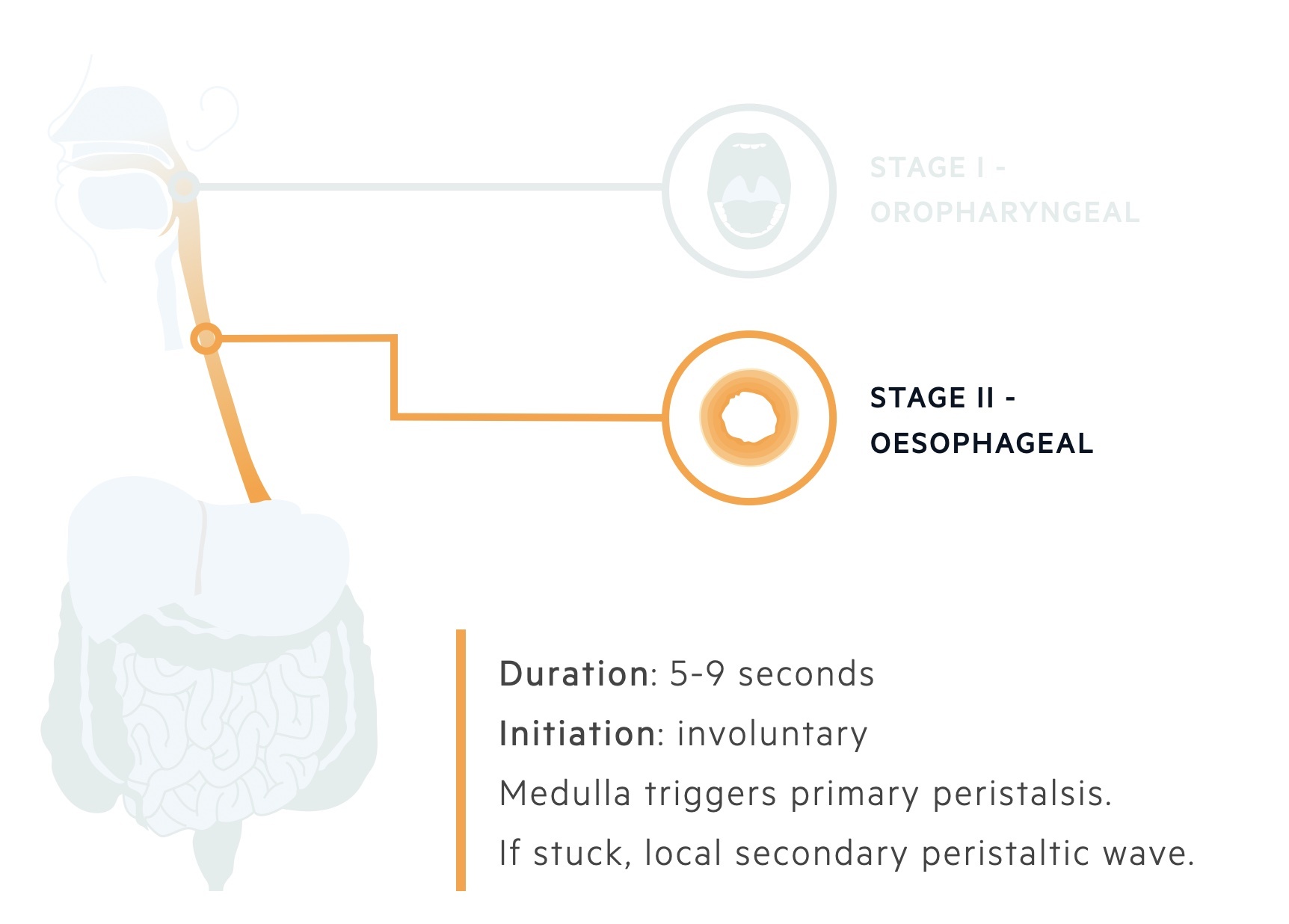
Deglutination
The process of swallowing is termed deglutination, and it is divided into two stages: oropharyngeal and oesophageal.
1. Oropharyngeal stage
The oropharyngeal stage of deglutination is a voluntarily initiated reflex, which takes approximately 1 second. It involves the movement of a bolus from the oral cavity to the oropharynx.
During the movement of this bolus a number of mechanisms help to prevent entry of the bolus into other passageways:
- The tongue prevents re-entry into the mouth.
- The soft palate prevents entry into nasal passages.
- Closure of rima glottis and movement of larynx prevents entry into the trachea. This is aided by the movement of the epiglottis over the closed glottis.
- The pharyngeal muscles contract to move the bolus to the top of the oesophagus.
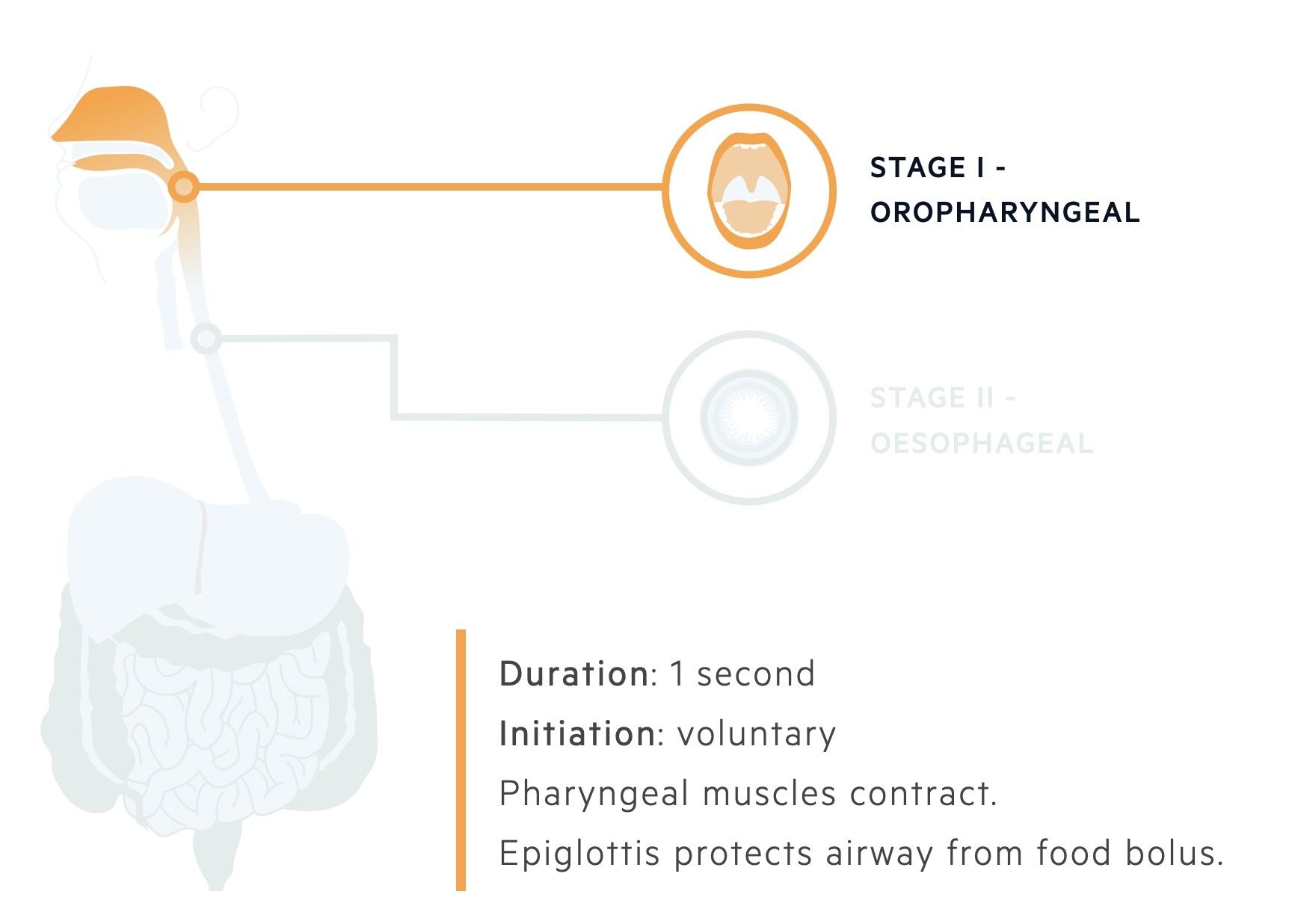
2. Oesophageal stage
The oesophageal stage of deglutination is initiated by the swallowing centre in the brain. This leads to the development of a primary peristaltic wave, which propels the bolus through the oesophagus. This stage of deglutination is involuntary and takes approximately 5-9 seconds.
The bolus passes from the top of the oesophagus to the gastro-oesophageal sphincter at the bottom of the oesophagus. If the bolus becomes stuck, a secondary peristaltic wave is generated locally to aid passage alongside an increase in salivary secretion.