Introduction
Diagnostic testing is based on the phenomenon that components of blood and other body fluids are found at different concentrations in individuals with a particular disease relative to people without the disease.
For instance, fasting blood glucose concentrations are raised in those who suffer from diabetes. Blood glucose concentration can therefore be used as a method for identifying undetected cases of diabetes in the population. In men, prostate specific antigen (PSA) levels in blood are higher on average in those who have prostate cancer and can be used to detect and manage progression of the disease.
In these notes, we will look at diagnostic tests including normal ranges, sensitivity, specificity, and positive and negative predictive values
Normal range
Many diagnostic tests are reported in relation to the ‘normal’ or ‘reference’ range.
This is a range in which the values for 95% (usually, but could be 90%) of people without the disease (normal individuals) are found. A test value outside the range may indicate a problem.
Diagnostic tests
Tests are usually based on diseased individuals having higher values than those who are disease-free; for some tests the reverse may be true.
Few tests are perfect. There will be disease-free individuals with a relatively large test value and diseased individuals with a relatively small test value leading to overlap between the distributions for the disease-free and diseased cases. This will produce some false positives (people who test positive but do not have the disease), and some false negatives (people who test negative but do have the disease).
By convention, test values indicating a raised chance of having the disease under investigation are referred to as positive test results, other results being referred to as negative test results.
A diagnostic test is assessed by its sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV).
Sensitivity & specificity
Both the sensitvity and specificity address the following question: “How good is the diagnostic test at identifying diseased and disease-free individuals?”
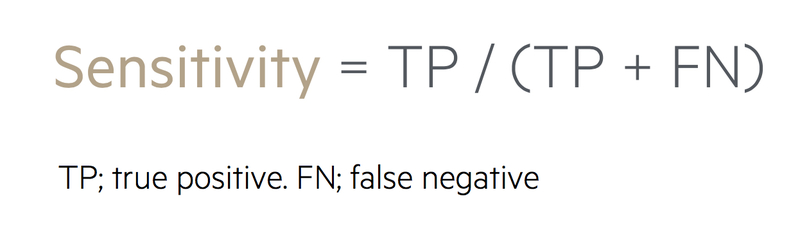
Sensitivity
This is equal to the proportion of people with the disease who are positive to the test
It is the ‘Number of diseased individuals positive to the test divided by the total number of diseased individuals’.
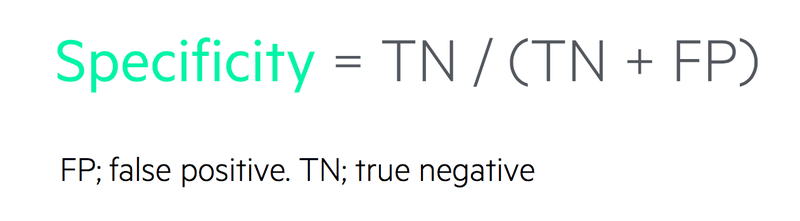
Specificity
This is equal to the proportion of disease-free people who are negative to the test
It is the ‘Number of diseased-free individuals negative to the test divided by the Total number of disease-free individuals’.
Positive predictive value
The positive predictive value is equal to the proportion of people out of those positive to the test who actually have the disease
It is the ‘Number of diseased individuals positive to the test divided by the total number of individuals positive to the test’.
The positive predictive value is concerned with the chance that someone has the disease given that they have received a positive diagnostic test result. For patients who have undergone diagnostic testing and received a positive result, this is their most important question.
Negative predictive value
The negative predictive value is equal to the proportion of people out of those negative to the test who are actually disease-free:
It is the ‘Number of diseased-free individuals negative to the test divided by the total number of individuals negative to the test’.

The negative predictive value addresses the question “What is the chance that a patient is disease-free given that they have received a negative diagnostic test result?” In this situation, the patient will be seeking reassurance.
From the clinician’s perspective, although reassurance should be the main aim, he or she should also explain that the disease could have remained undetected. In addition, the patient should be aware that the disease might develop in the future irrespective of their medical history to date.
Likelihood ratios
Some diagnostic studies additionally report findings in terms of likelihood ratios.
For a positive test, the likelihood ratio is the probability of testing positive for those with the disease, divided by the probability of testing positive for those without the disease. It is equal to the sensitivity/(1-specificity).
Similarly the likelihood ratio for a negative test is the probability of testing negative for those with the disease, divided by the probability of testing negative for the disease-free group or (1-sensitivity)/specificity.
Ethical considerations
Patients should undergo diagnostic testing only in clinically appropriate situations.
Diagnostic tests ought not be used in a general search for possible medical diagnoses. The patient needs to be fully informed of the advantages and disadvantages of the diagnostic test before making a final decision on whether or not to go ahead. The discussion should involve the patients, clinicians and significant individuals in the patient’s life such as family and friends. When things go wrong, legal challenges are not unknown.
An individual who does not have the disease but receives a positive test result risks needless worry and unnecessary further investigations. A diseased individual who receives a negative test result may receive false reassurance and consequently raised hopes.
Once the disease is finally detected in such individuals, the subsequent treatment may be more costly and have poorer prognosis than it might have been starting from a correct diagnostic test result.
As with all other aspects of patient care, strict confidentiality should be maintained and information should be released selectively on a need-to-know basis.


