Definition & classification
Aortic stenosis refers to obstruction of blood flow across the aortic valve, typically due to calcification.
Aortic stenosis is the most common valvular disease in the Europe and North America. It affects between 2-7% of those over 65 and symptomatic disease affects men four times more frequently than women. Typically a disease of the elderly, presenting in the seventh or eighth decades of life.
Aetiology
Calcification is the most common cause of aortic stenosis in the western world.
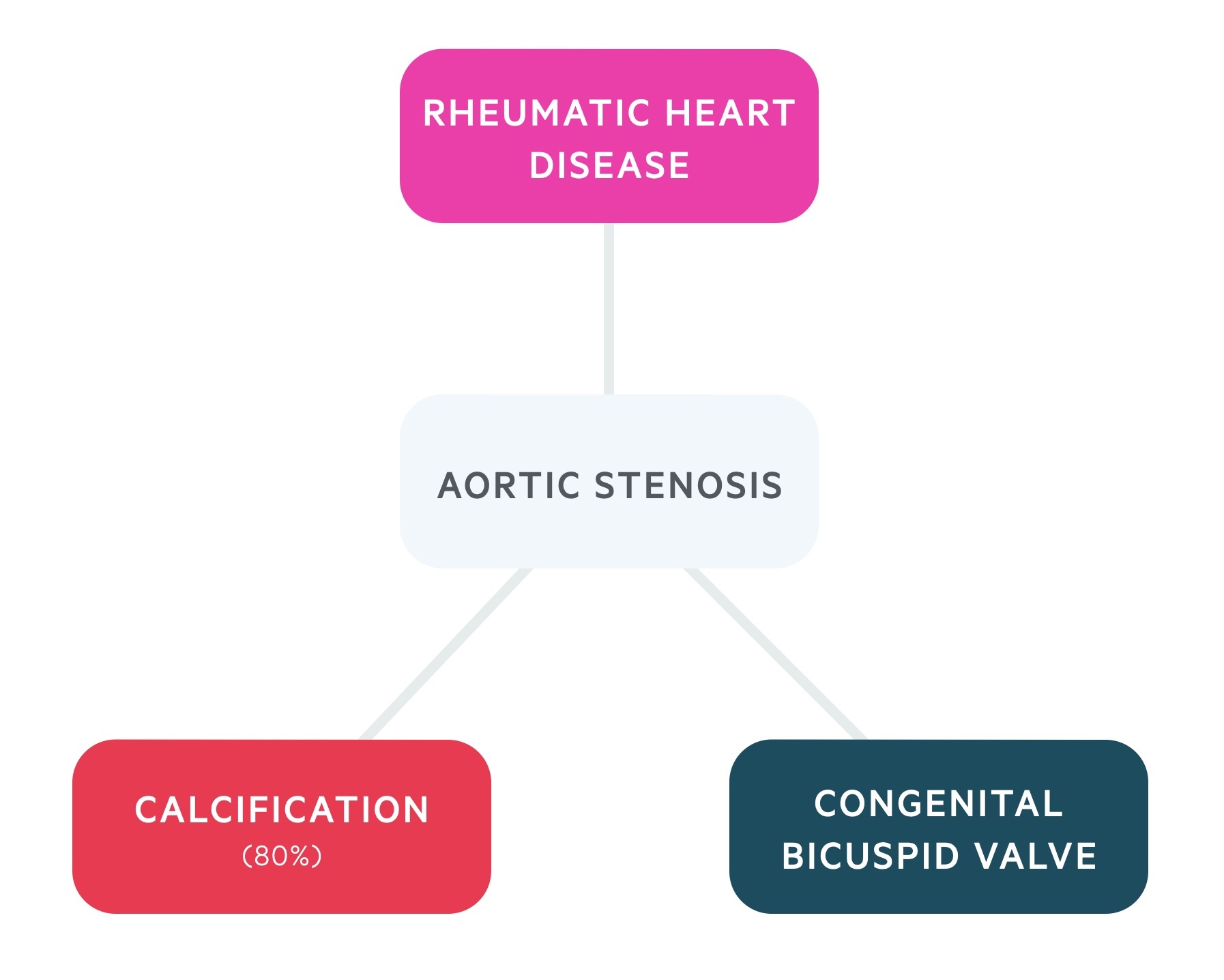
1. Calcific (degenerative)
A degenerative condition caused by inflammation and progressive calcification which limits movement of the aortic valve.
- Most common cause (80%).
- Affects patients later in life (>65).
- Risk factors: hypercholesterolaemia, hypertension, smoking and diabetes.
2. Bicuspid valve (congenital)
The most common congenital abnormality of the heart occurring with a frequency of 1-2%, with males more commonly affected.
- Valves predisposed to becoming stenotic.
- Stenosis tends to appear at a younger age (<65).
- Abnormal valve leads to turbulent flow with subsequent fibrosis and calcification.
3. Rheumatic heart disease
An autoimmune condition that follows streptococcal (Group A) infection.
- Inflammation is a result of molecular mimicry.
- Tissues affected include heart, joints and CNS.
- Becoming increasingly uncommon.
Pathophysiology
Aortic stenosis places pressure on the left ventricle; in response it undergoes hypertrophy.
Aortic stenosis is a problem of left ventricular outflow. A pressure gradient develops across the valve (hence, an ejection systolic murmur may be heard).
Initially, this leads to systolic dysfunction, the heart can not pump out a normal proportion of its end-diastolic volume. Compensatory mechanisms result in left ventricular (concentric) hypertrophy – hence, a sustained apex. This hypertrophy may eventually lead to diastolic dysfunction through impaired relaxation and reduced compliance.
Cardiac failure ensues with features of left-sided heart failure. Features include shortness of breath (dyspnoea) and bibasal crackles. Patients have a reduced ability to adjust to increased myocardial demands as they exhaust compensatory mechanisms. As such patients become prone to exertional syncope.
Angina may develop for a number of reasons:
- Reduced coronary flow
- Increased oxygen requirements (from hypertrophied cardiac muscle)
- Concomitant coronary artery disease
Clinical features
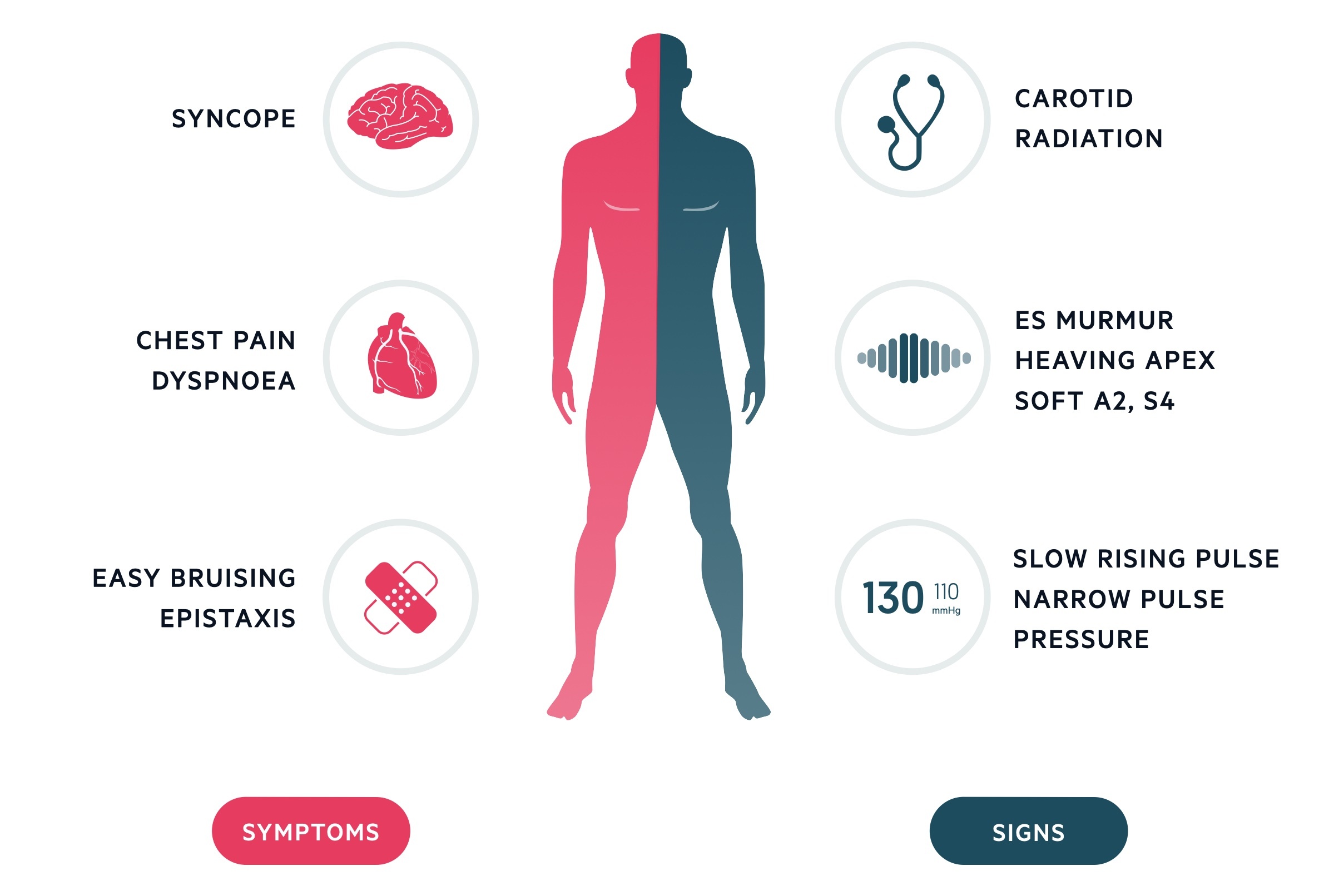
A classical triad of ‘SAD‘ is often described.
Symptoms
- Syncope (exertional)
- Angina
- Dyspnoea
The classical triad is only seen in around 40-50% of patients. Patients may also complain of epistaxis or bruising. Turbulent flow across the stenotic aortic valve can lead to an acquired von Willebrand deficiency, with high shear forces inducing structural changes in the shape of the protein leading to clotting abnormalities.
Signs
- Ejection systolic murmur, radiating to the carotids.
- Sustained apex
- Slow rising pulse
- Narrow pulse pressure
- Others:
- Soft S2 – a marker of severity, the aortic component of the second heart sound may become quieter in more severe disease as the valve leaflets fail to oppose each other forcefully.
- Fourth heart sound (S4) – caused by the atria contracting against stiff, hypertrophied ventricles.
- Reversed splitting
Investigations & diagnosis
Echocardiogram is used to diagnose aortic stenosis.
Bedside
- Observations
- Blood pressure
- ECG
- Left ventricular hypertrophy (deep S-waves in V1 and V2, tall R-waves in V5 and V6).
- Left ventricular strain may be seen in severe disease.
Bloods
- FBC
- U&Es
- Cholesterol
- Clotting
Imaging
- CXR
- Typically demonstrates a small heart; cardiomegaly occurs if heart failure develops.
- Dilated ascending aorta.
- Echocardiogram
- Allows assessment of the valve area, ejection fraction and ventricular hypertrophy.
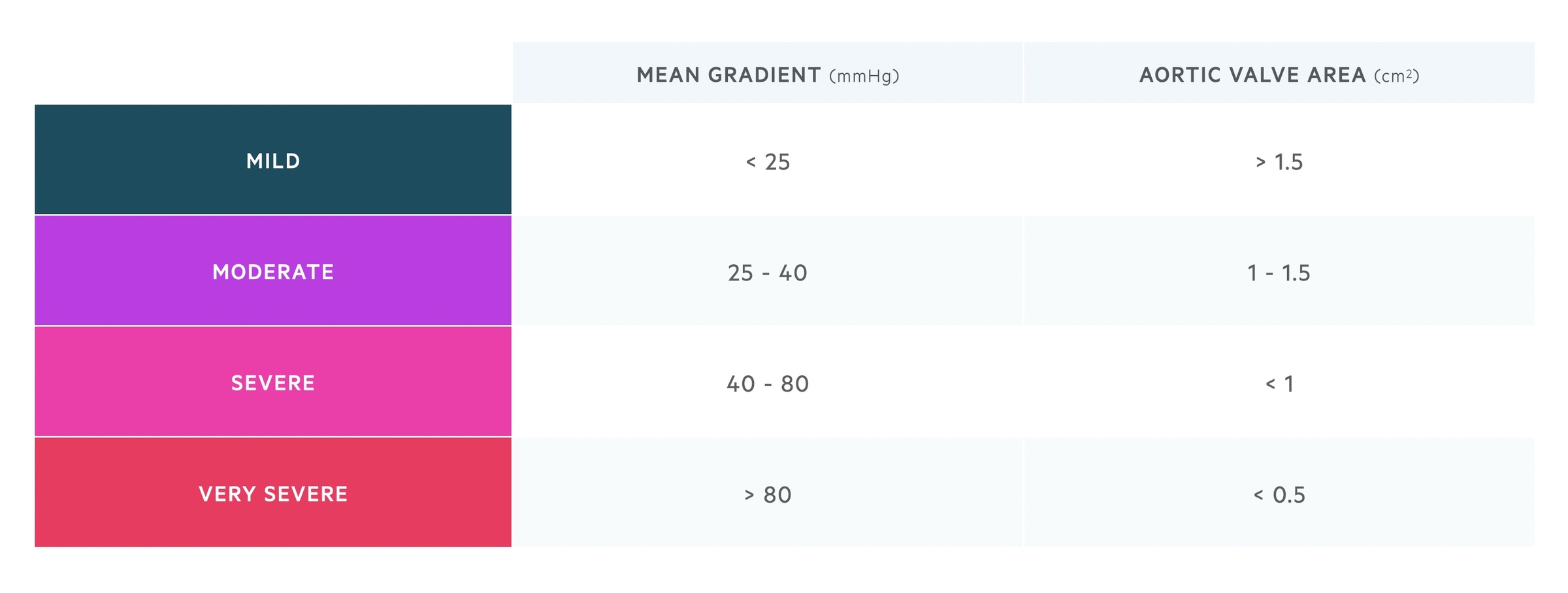
- Aortic stenosis is classified by severity on echocardiogram according to its transaortic pressure gradient & valve area.
Special
- Cardiac MRI
- Cardiac catheterisation
- ECG exercise stress testing
- May be used in asymptomatic patients. A positive test may be indicated by the onset of symptoms, ECG changes, or an abnormal BP response.
Management
Surgical aortic valve replacement is indicated in severe or symptomatic disease. Severity is indicated on echo by LVH, pressure gradient and valve area. Successful surgery leads to much improved quality of life.
Valvotomy
Stenotic lesions may be treated with a valvotomy, a procedure in which the stenotic valve leaflets are forced apart, it may be:
- Percutaneous balloon valvotomy
- Open valvotomy
Valve replacement
- Mechanical valve – require long-term anticoagulation, long lifespan reducing the need for a second operation. Suited to younger patients.
- Bioprosthetic valve – no need for long-term anticoagulation, limited life span (around 10 years) and a repeat operation is more likely. Suited to older patients.
The decision of mechanical vs bioprosthetic valve should take into account patient-specific factors and wishes. Traditionally valve replacement has necessitated open surgery, novel techniques now allow percutaneous replacement: transcatheter aortic valve replacement (TAVR) – a minimally invasive technique that utilises an expandable valve, may be used in patients who are not candidates for open surgery.
Coronary angiogram may be used to demonstrate atherosclerotic disease that may be treated with CABG at the same time as the open surgery.

